Hisert Katherine B, Birkland Timothy P, Schoenfelt Kelly Q, Long Matthew E, Grogan Brenda, Carter Suzanne, Liles W Conrad, McKone Edward F, Becker Lev, Manicone Anne M, Gharib Sina A
Division of Pulmonary, Critical Care, and Sleep Medicine, Department of Medicine, National Jewish Health, Denver, CO, United States.
Center for Lung Biology, Division of Pulmonary, Critical Care, and Sleep Medicine, Department of Medicine, University of Washington, Seattle, WA, United States.
Front Pharmacol. 2020 Aug 13;11:1219. doi: 10.3389/fphar.2020.01219. eCollection 2020.
CFTR modulators decrease some etiologies of CF airway inflammation; however, data indicate that non-resolving airway infection and inflammation persist in individuals with CF and chronic bacterial infections. Thus, identification of therapies that diminish airway inflammation without allowing unrestrained bacterial growth remains a critical research goal. Novel strategies for combatting deleterious airway inflammation in the CFTR modulator era require better understanding of cellular contributions to chronic CF airway disease, and how inflammatory cells change after initiation of CFTR modulator therapy. Peripheral blood monocytes, which traffic to the CF airway, can develop both pro-inflammatory and inflammation-resolving phenotypes, represent intriguing cellular targets for focused therapies. This therapeutic approach, however, requires a more detailed knowledge of CF monocyte cellular programming and phenotypes.
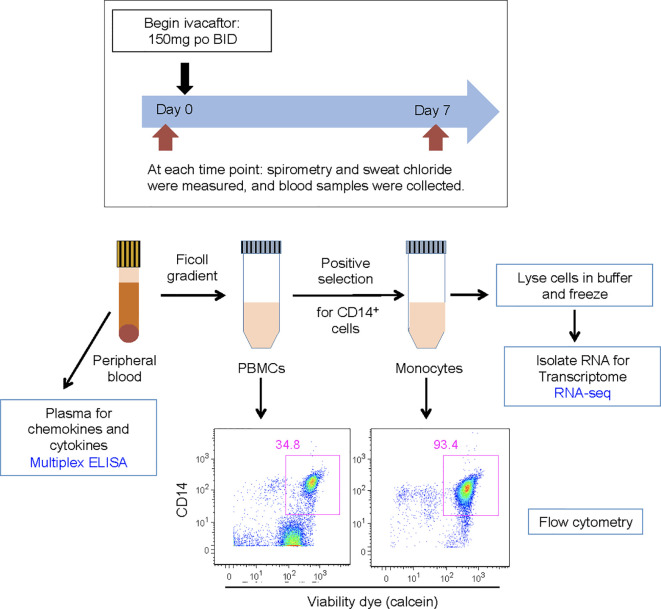
In order to characterize the inflammatory phenotype of CF monocytes, and how these cells change after initiation of CFTR modulator therapy, we studied adults (n=10) with CF, chronic airway infections, and the mutations before and 7 days after initiation of ivacaftor. Transcriptomes of freshly isolated blood monocytes were interrogated by RNA-sequencing (RNA-seq) followed by pathway-based analyses. Plasma concentrations of cytokines and chemokines were evaluated by multiplex ELISA.
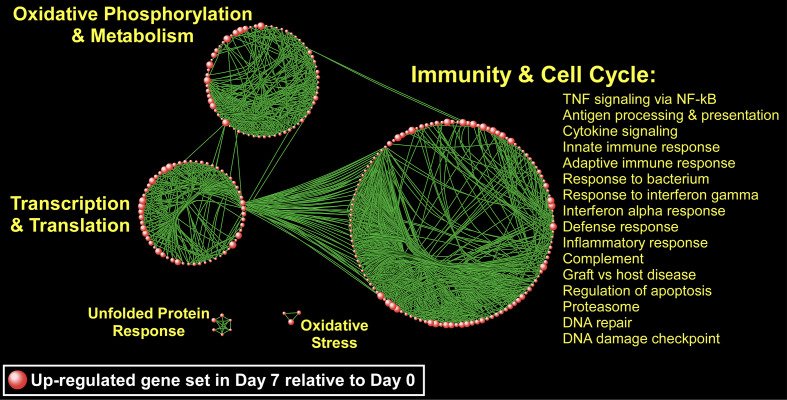
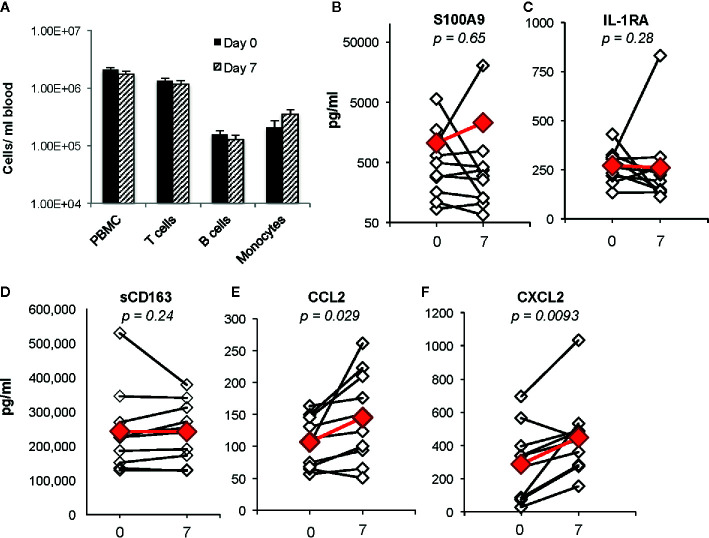
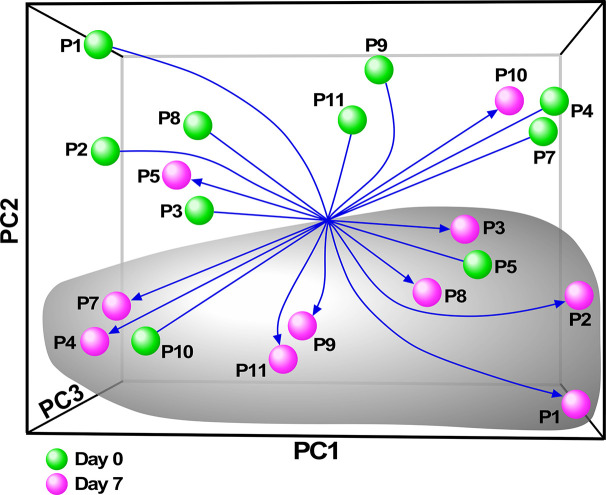
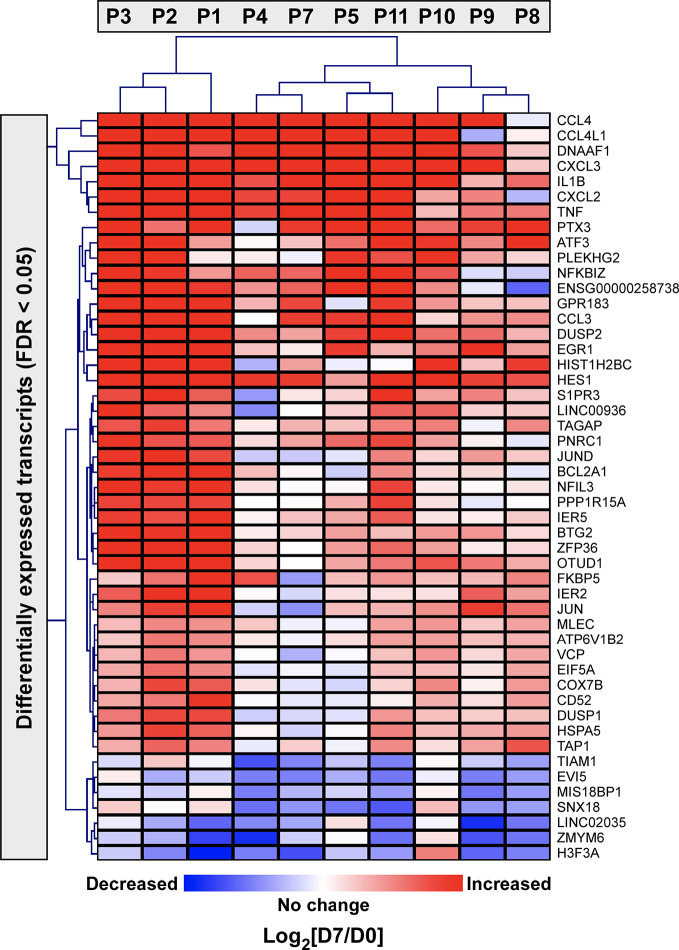
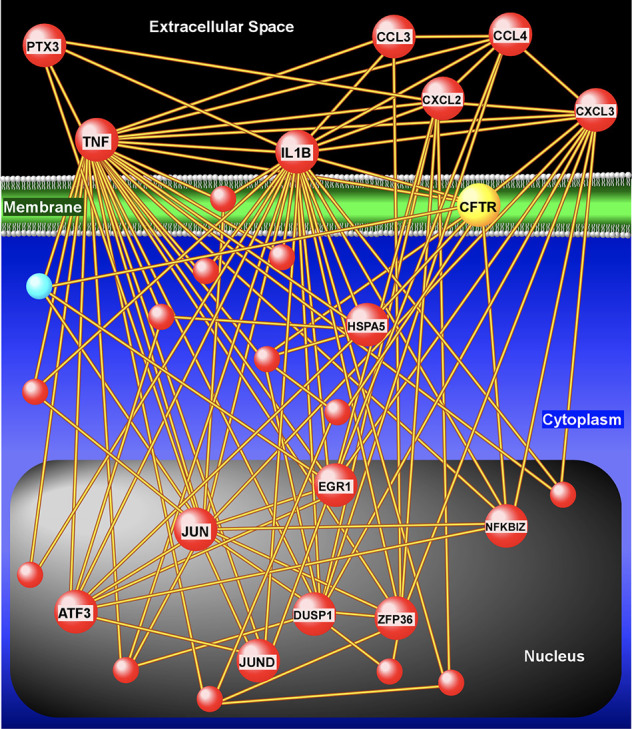
RNAseq identified approximately 50 monocyte genes for which basal expression was significantly changed in all 10 subjects after 7 days of ivacaftor. Of these, the majority were increased in expression post ivacaftor, including many genes traditionally associated with enhanced inflammation and immune responses. Pathway analyses confirmed that transcriptional programs were overwhelmingly up-regulated in monocytes after 7 days of ivacaftor, including biological modules associated with immunity, cell cycle, oxidative phosphorylation, and the unfolded protein response. Ivacaftor increased plasma concentrations of CXCL2, a neutrophil chemokine secreted by monocytes and macrophages, and CCL2, a monocyte chemokine.
Our results demonstrate that ivacaftor causes acute changes in blood monocyte transcriptional profiles and plasma chemokines, and suggest that increased monocyte inflammatory signals and changes in myeloid cell trafficking may contribute to changes in airway inflammation in people taking CFTR modulators. To our knowledge, this is the first report investigating the transcriptomic response of circulating blood monocytes in CF subjects treated with a CFTR modulator.
囊性纤维化跨膜传导调节因子(CFTR)调节剂可减轻囊性纤维化(CF)气道炎症的某些病因;然而,数据表明,CF患者以及慢性细菌感染患者中,气道感染和炎症持续存在且无法消退。因此,确定既能减轻气道炎症又不会导致细菌不受控制地生长的治疗方法仍然是一个关键的研究目标。在CFTR调节剂时代,对抗有害气道炎症的新策略需要更好地了解细胞对慢性CF气道疾病的影响,以及CFTR调节剂治疗开始后炎症细胞如何变化。外周血单核细胞可迁移至CF气道,能产生促炎和抗炎两种表型,是靶向治疗的有趣细胞靶点。然而,这种治疗方法需要更详细地了解CF单核细胞的细胞编程和表型。
为了表征CF单核细胞的炎症表型,以及这些细胞在CFTR调节剂治疗开始后如何变化,我们研究了10名患有CF、慢性气道感染且携带特定突变的成年人,在给予依伐卡托治疗前和治疗7天后进行研究。通过RNA测序(RNA-seq)对新鲜分离的血液单核细胞的转录组进行分析,随后进行基于通路的分析。通过多重ELISA评估细胞因子和趋化因子的血浆浓度。
RNA测序确定了大约50个单核细胞基因,在依伐卡托治疗7天后,所有10名受试者的这些基因的基础表达均发生了显著变化。其中,大多数基因在依伐卡托治疗后表达增加,包括许多传统上与炎症和免疫反应增强相关的基因。通路分析证实,依伐卡托治疗7天后,单核细胞中的转录程序绝大多数上调,包括与免疫、细胞周期、氧化磷酸化和未折叠蛋白反应相关的生物学模块。依伐卡托增加了CXCL2(一种由单核细胞和巨噬细胞分泌的中性粒细胞趋化因子)和CCL2(一种单核细胞趋化因子)的血浆浓度。
我们的结果表明,依伐卡托会导致血液单核细胞转录谱和血浆趋化因子发生急性变化,并表明单核细胞炎症信号增加和髓样细胞迁移变化可能导致服用CFTR调节剂的患者气道炎症发生变化。据我们所知,这是第一份研究CFTR调节剂治疗的CF患者循环血液单核细胞转录组反应的报告。