St. Joseph's University Hospital, Paterson, NJ, United States.
Texas Children's Hospital, Balor College of Medicine, Houston, TX, United States.
Front Immunol. 2020 Sep 4;11:1929. doi: 10.3389/fimmu.2020.01929. eCollection 2020.
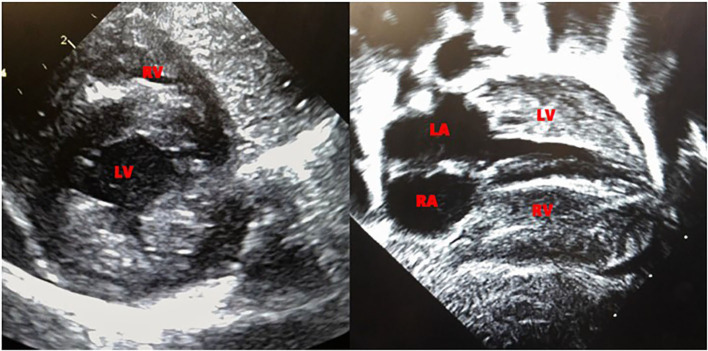
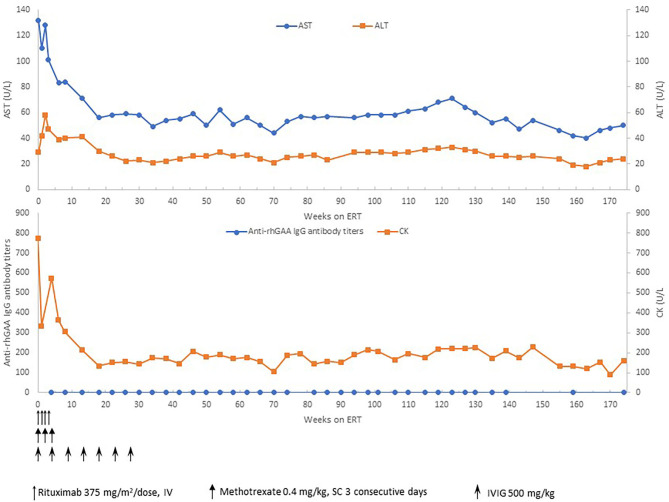
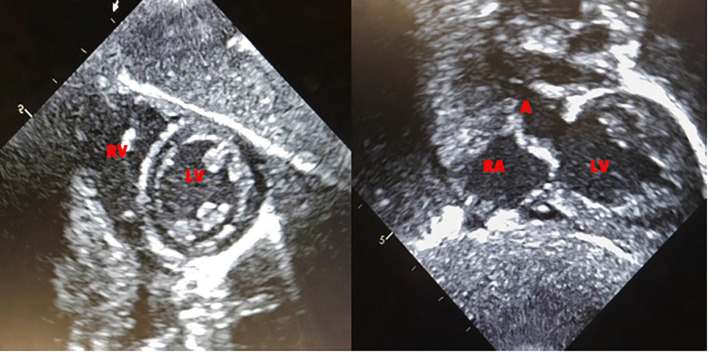
We report the clinical course of the first prenatally diagnosed cross-reactive immunologic material (CRIM)-negative infantile Pompe disease (IPD) patient [homozygous for c.2560C>T (p.Arg854X) variant in the gene] to undergo prophylactic immune tolerance induction (ITI) and enzyme replacement therapy (ERT) within the first 2 days of life. Both parents were found to be carriers of the c.2560C>T (p.Arg854X) variant through prenatal carrier screening. Fetal echocardiogram at 31 weeks of gestation showed left ventricular hypertrophy. An echocardiogram on the 1st day of life revealed marked biventricular hypertrophy. Physical exam was significant for macroglossia and hypotonia. A short course of Prophylactic ITI with rituximab, methotrexate, and intravenous immunoglobulin (IVIG) in conjunction with ERT at a dose of 20 mg/kg every other week was started on day 2 of life. The patient completed the ITI protocol safely and complete B-cell recovery, based on CD19 count, was noted by 3 months of age. The patient never developed anti-rhGAA IgG antibodies to ERT. Vaccinations were initiated at 9 months of age, with adequate response noted. Complete recovery of cardiac function and left ventricular mass was seen by 11 weeks of age. At 8 months of age, the patient developmentally measured at 75-90% on the Alberta Infant Motor Scale, walked at 11 months and continues to develop age-appropriately at 50 months of age based on the Early Learning Accomplishment Profile. ERT dosing was increased to 40 mg/kg every 2 weeks at 32 months of age and frequency increased to 40 mg/kg every week at 47 months of age. Patient continues to have undetectable antibody titers, most recently at age 50 months and urine Hex4 has remained normal. To our knowledge, this is the first report of successful early ERT and ITI in a prenatally diagnosed CRIM-negative IPD patient and the youngest IPD patient to receive ITI safely. With the addition of Pompe disease to the Recommended Uniform Screening Panel(RUSP) and its addition to multiple state newborn screening programs, our case highlights the benefits of early diagnosis and timely initiation of treatment in babies with Pompe disease, who represent the most severe end of the disease spectrum.
我们报告了首例产前诊断为交叉反应免疫物质(CRIM)阴性婴儿庞贝病(IPD)患者[基因中 c.2560C>T(p.Arg854X)变体纯合子]的临床病程,该患者在出生后 2 天内接受了预防性免疫耐受诱导(ITI)和酶替代治疗(ERT)。通过产前携带者筛查发现,父母双方均为 c.2560C>T(p.Arg854X)变体携带者。31 周胎儿超声心动图显示左心室肥厚。出生后第 1 天的超声心动图显示明显的双心室肥厚。体格检查发现巨舌和低张力。短期的 ITI 治疗方案为利妥昔单抗、甲氨蝶呤和静脉免疫球蛋白(IVIG)联合 ERT,剂量为 20mg/kg,每两周一次,于出生后第 2 天开始。患者安全完成 ITI 方案,根据 CD19 计数,在 3 个月时观察到完全 B 细胞恢复。患者从未对 ERT 产生抗 rhGAA IgG 抗体。患者在 9 个月时开始接种疫苗,观察到充分的反应。出生后 11 周时,心脏功能和左心室质量完全恢复。在 8 个月大时,患者在阿尔伯塔婴儿运动量表上的发育测量值为 75-90%,在 11 个月大时会走路,并在 50 个月大时根据早期学习成就档案继续以适合年龄的方式发展。在 32 个月大时,ERT 剂量增加到 40mg/kg,每两周一次,在 47 个月大时增加到每周 40mg/kg。患者的抗体滴度仍未检出,最近一次检测是在 50 个月大时,尿液 Hex4 也一直正常。据我们所知,这是首例成功的产前诊断为 CRIM 阴性 IPD 患者的早期 ERT 和 ITI 报告,也是接受 ITI 治疗的最小 IPD 患者。随着庞贝病被添加到推荐的统一筛查面板(RUSP)中,并被添加到多个州的新生儿筛查计划中,我们的病例强调了在婴儿期早期诊断和及时开始治疗的益处,这些婴儿代表了疾病谱的最严重端。