Division of Pediatric Critical Care Medicine, Department of Pediatrics, Washington University School of Medicine, St. Louis, MO, United States.
Section of Acute and Critical Care Surgery, Department of Surgery, Washington University School of Medicine, St. Louis, MO, United States.
Front Immunol. 2020 Sep 8;11:2085. doi: 10.3389/fimmu.2020.02085. eCollection 2020.
The hemostatic properties of tranexamic acid (TXA) are well described, but the immunological effects of TXA administration after traumatic injury have not been thoroughly examined. We hypothesized TXA would reduce monocyte activation in bleeding trauma patients with severe injury.
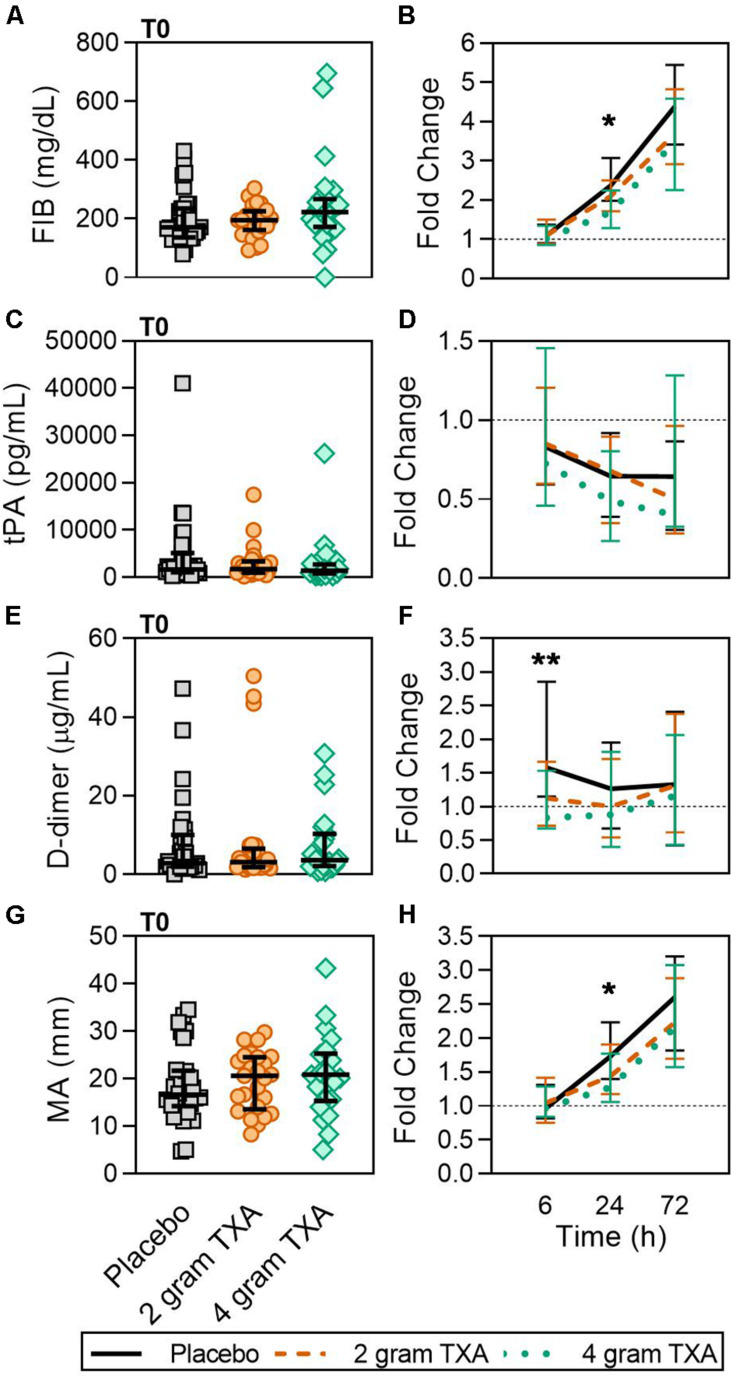
This was a single center, double-blinded, randomized controlled trial (RCT) comparing placebo to a 2 g or 4 g intravenous TXA bolus dose in trauma patients with severe injury. Fifty patients were randomized into each study group. The primary outcome was a reduction in monocyte activation as measured by human leukocyte antigen-DR isotype (HLA-DR) expression on monocytes 72 h after TXA administration. Secondary outcomes included kinetic assessment of immune and hemostatic phenotypes within the 72 h window post-TXA administration.
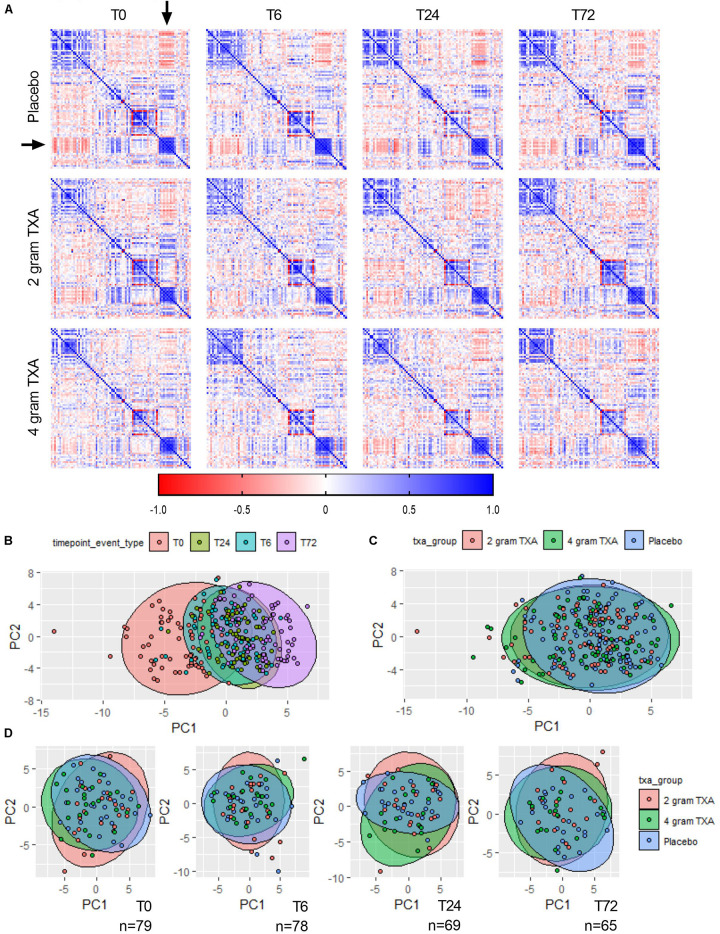
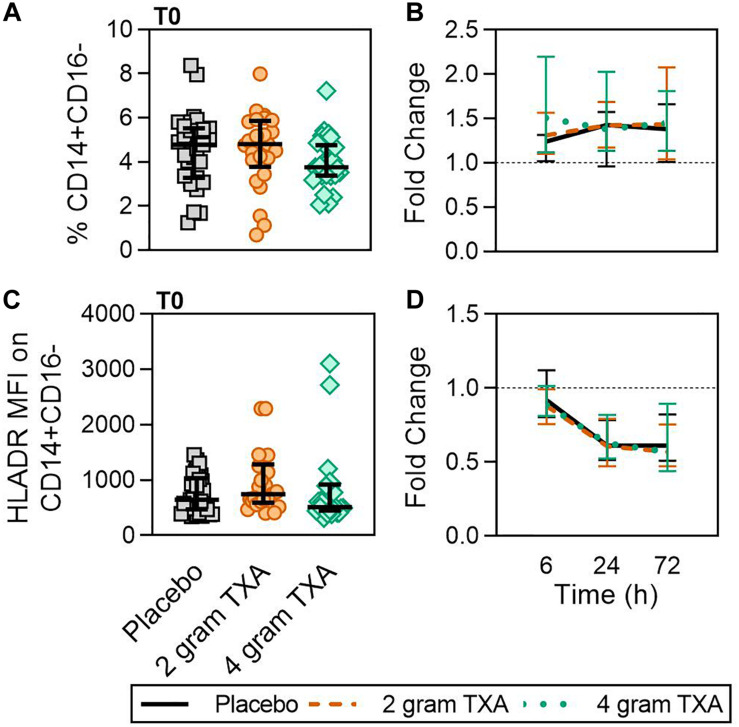
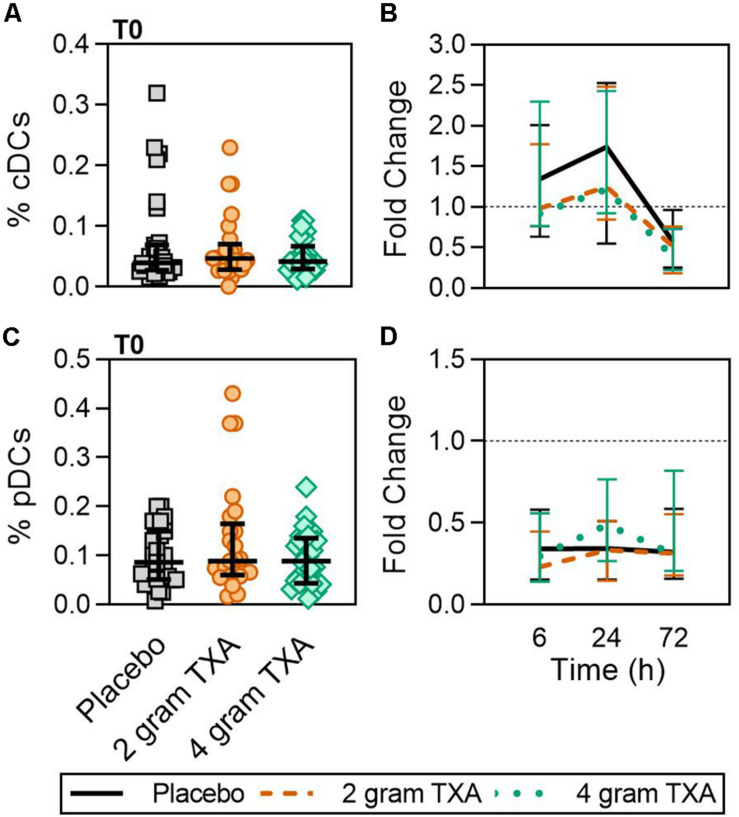
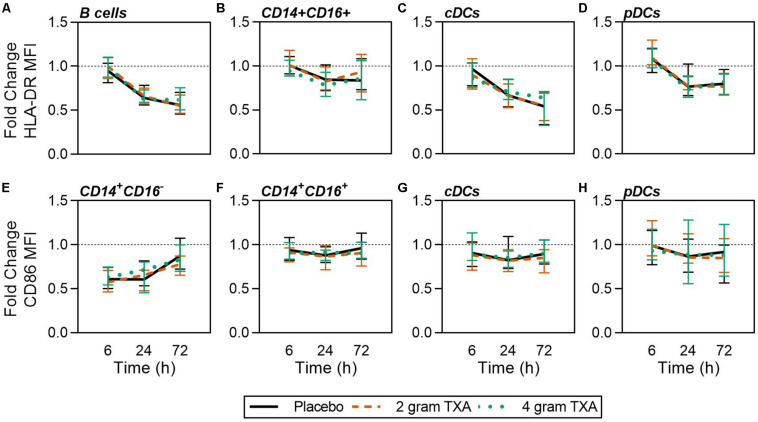
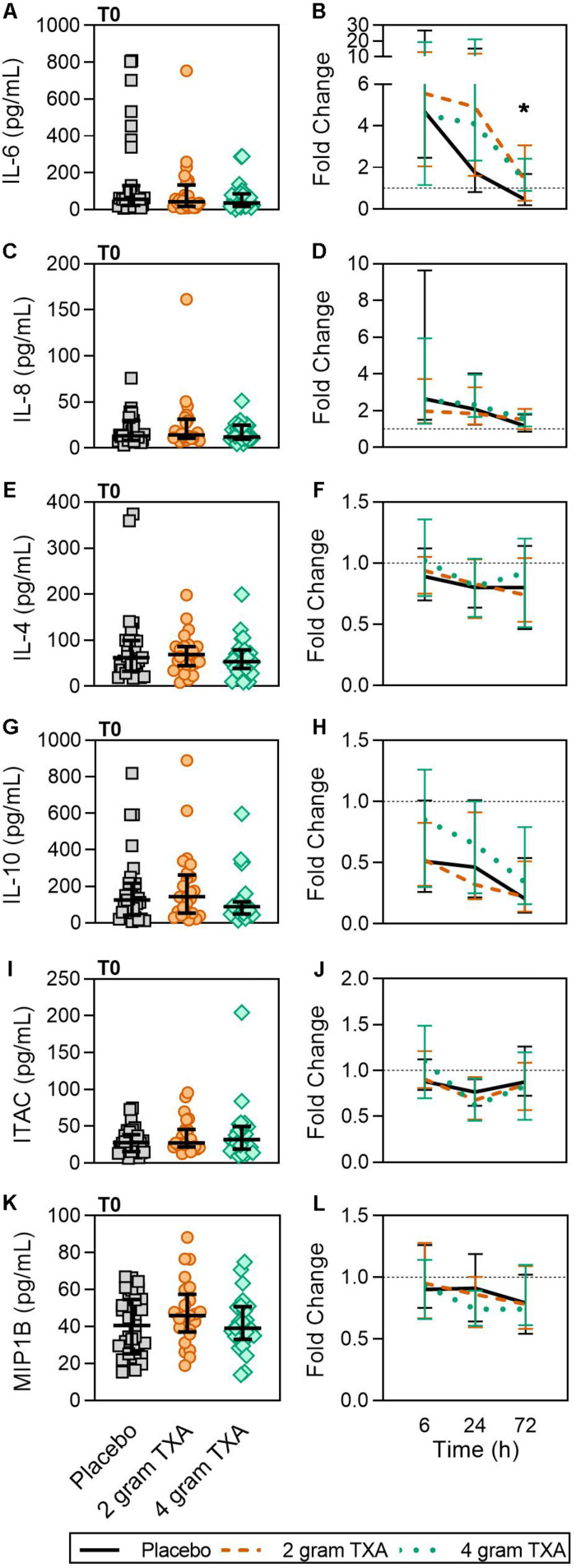
The trial occurred between March 2016 and September 2017, when data collection ended. 149 patients were analyzed (placebo, = 50; 2 g TXA, = 49; 4 g TXA, = 50). The fold change in HLA-DR expression on monocytes [reported as median (Q1-Q3)] from pre-TXA to 72 h post-TXA was similar between placebo [0.61 (0.51-0.82)], 2 g TXA [0.57 (0.47-0.75)], and 4 g TXA [0.57 (0.44-0.89)] study groups ( = 0.82). Neutrophil CD62L expression was reduced in the 4 g TXA group [fold change: 0.73 (0.63-0.97)] compared to the placebo group [0.97 (0.78-1.10)] at 24 h post-TXA ( = 0.034). The fold decrease in plasma IL-6 was significantly less in the 4 g TXA group [1.36 (0.87-2.42)] compared to the placebo group [0.46 (0.19-1.69)] at 72 h post-TXA ( = 0.028). There were no differences in frequencies of myeloid or lymphoid populations or in classical complement activation at any of the study time points.
In trauma patients with severe injury, 4 g intravenous bolus dosing of TXA has minimal immunomodulatory effects with respect to leukocyte phenotypes and circulating cytokine levels.
www.ClinicalTrials.gov, identifier NCT02535949.
氨甲环酸(TXA)具有良好的止血特性,但 TXA 在创伤后给药的免疫效应尚未得到彻底研究。我们假设 TXA 会减少严重创伤出血患者单核细胞的激活。
这是一项单中心、双盲、随机对照试验(RCT),比较了严重创伤患者接受安慰剂与 2 g 或 4 g 静脉 TXA 推注剂量的效果。每组 50 名患者被随机分配到研究组。主要结局是通过单核细胞 HLA-DR 同种型(HLA-DR)表达在 TXA 给药后 72 小时测量单核细胞的激活减少。次要结局包括在 TXA 给药后 72 小时内对免疫和止血表型的动力学评估。
试验于 2016 年 3 月至 2017 年 9 月进行,数据收集结束。分析了 149 名患者(安慰剂组 = 50 例;2 g TXA 组 = 49 例;4 g TXA 组 = 50 例)。从 TXA 前到 72 小时,单核细胞 HLA-DR 表达的倍数变化[中位数(Q1-Q3)]在安慰剂组[0.61(0.51-0.82)]、2 g TXA 组[0.57(0.47-0.75)]和 4 g TXA 组[0.57(0.44-0.89)]相似( = 0.82)。与安慰剂组[0.97(0.78-1.10)]相比,4 g TXA 组在 TXA 后 24 小时[折叠变化:0.73(0.63-0.97)]中性粒细胞 CD62L 表达减少( = 0.034)。与安慰剂组[0.46(0.19-1.69)]相比,4 g TXA 组在 TXA 后 72 小时[折叠减少:1.36(0.87-2.42)]血浆 IL-6 的减少明显减少( = 0.028)。在任何研究时间点,髓样或淋巴样群体的频率或经典补体激活均无差异。
在严重创伤患者中,4 g 静脉推注 TXA 对白细胞表型和循环细胞因子水平的免疫调节作用最小。
www.ClinicalTrials.gov,标识符 NCT02535949。