Suzuki Eiji, Ichimura Takuya, Kimura Satoru, Kanno Takashi, Migita Kiyoshi
Department of Rheumatology, Ohta-Nishinouchi Hospital, 2-5-20, Nishinouchi, Koriyama City, Fukushima 963-8558, Japan.
Department of Hematology, Ohta-Nishinouchi Hospital, 2-5-20, Nishinouchi, Koriyama City, Fukushima 963-8558, Japan.
Case Rep Rheumatol. 2020 Sep 17;2020:8872774. doi: 10.1155/2020/8872774. eCollection 2020.
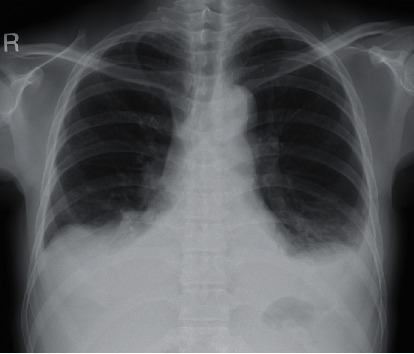
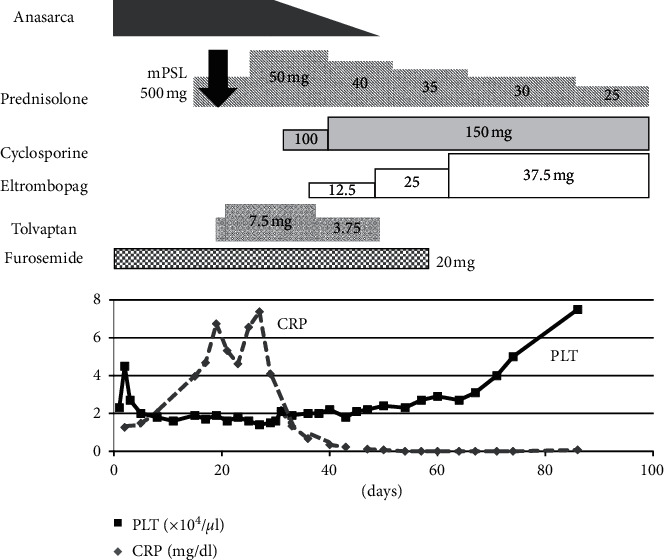
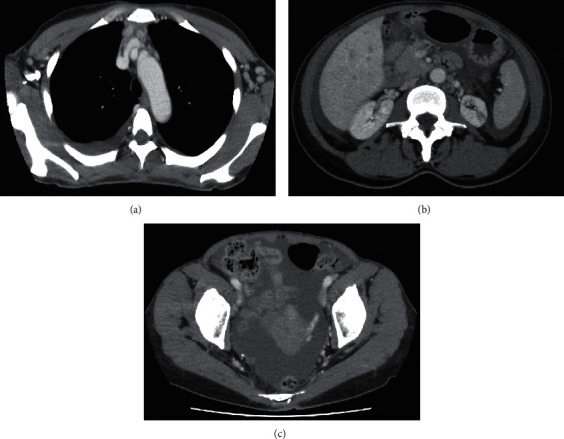
Sjögren's syndrome (SS) is associated with not only sicca symptoms but also various symptoms caused by extraglandular manifestation. The pathophysiology and comorbidities of TAFRO syndrome (thrombocytopenia, anasarca, fever, reticulin fibrosis, and organomegaly), which is thought to be a variant of multicentric Castleman's disease, are not fully understood, and there are few data on the effectiveness of treatments. We report a patient of SS with TAFRO syndrome-like clinical features. A 52-year-old woman was admitted to our hospital because of abdominal distension. Laboratory data showed thrombocytopenia, and image findings showed massive ascites without evidence of malignant disease as confirmed by cytology. She was diagnosed with SS based on dysfunction of salivary secretion and positivity for anti-Ro/SS-A and La/SS-B antibodies, accompanied by clinical features of TAFRO syndrome based on the presence of anasarca and thrombocytopenia. High-dose corticosteroid for inflammation, anasarca, and thrombocytopenia was not effective. Cyclosporine was administered next, but anasarca and thrombocytopenia did not immediately improve until tolvaptan and eltrombopag were added. Although tolvaptan and eltrombopag were used for only a few months, the patient maintained a good condition with cyclosporine and low-dose prednisolone. In SS patients, activation of antigen-specific T lymphocytes is thought to be an important trigger that accelerates the immune response and is followed by hypercytokinemia. Therefore, using cyclosporine to suppress the activity of T lymphocytes is a reasonable treatment for SS accompanied with TAFRO syndrome-like pathophysiology. It might also be useful to administer tolvaptan or eltrombopag before the effects of immunosuppressants appear. If refractory inflammation with anasarca, thrombocytopenia, or lymphadenopathy is observed in an SS patient, complications with TAFRO syndrome-like pathophysiology should be considered.
干燥综合征(SS)不仅与口干眼干症状有关,还与腺体外表现引起的各种症状相关。TAFRO综合征(血小板减少、全身性水肿、发热、网状纤维增生和器官肿大)被认为是多中心Castleman病的一种变体,其病理生理学和合并症尚未完全明确,关于治疗效果的数据也很少。我们报告了一名具有TAFRO综合征样临床特征的SS患者。一名52岁女性因腹胀入院。实验室数据显示血小板减少,影像学检查发现大量腹水,细胞学检查证实无恶性疾病迹象。根据唾液分泌功能障碍以及抗Ro/SS-A和La/SS-B抗体阳性,她被诊断为SS,并伴有全身性水肿和血小板减少的TAFRO综合征临床特征。用于治疗炎症、全身性水肿和血小板减少的高剂量皮质类固醇无效。接下来给予环孢素,但直到添加托伐普坦和艾曲泊帕,全身性水肿和血小板减少才立即改善。尽管托伐普坦和艾曲泊帕仅使用了几个月,但患者在使用环孢素和低剂量泼尼松龙的情况下保持良好状态。在SS患者中,抗原特异性T淋巴细胞的激活被认为是加速免疫反应并随后导致高细胞因子血症的重要触发因素。因此,使用环孢素来抑制T淋巴细胞的活性对于伴有TAFRO综合征样病理生理学的SS是一种合理的治疗方法。在免疫抑制剂起效之前给予托伐普坦或艾曲泊帕可能也有用。如果在SS患者中观察到伴有全身性水肿、血小板减少或淋巴结病的难治性炎症,应考虑TAFRO综合征样病理生理学的并发症。