Davenport Matthew S, Perazella Mark A, Yee Jerry, Dillman Jonathan R, Fine Derek, McDonald Robert J, Rodby Roger A, Wang Carolyn L, Weinreb Jeffrey C
Department of Radiology, Michigan Medicine, Ann Arbor, MI.
Department of Urology, Michigan Medicine, Ann Arbor, MI.
Kidney Med. 2020 Jan 22;2(1):85-93. doi: 10.1016/j.xkme.2020.01.001. eCollection 2020 Jan-Feb.
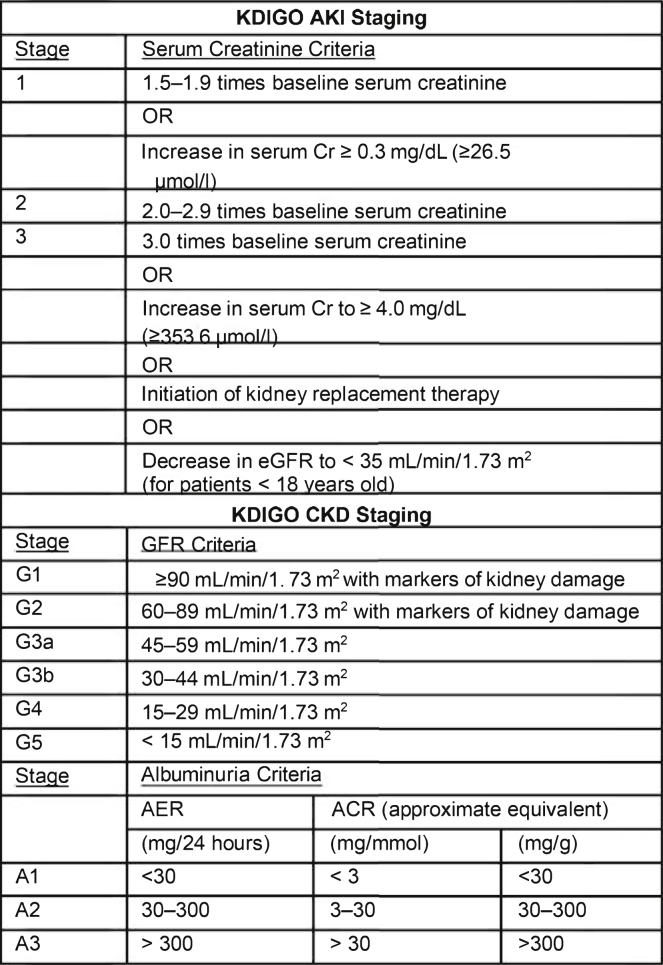
Intravenous iodinated contrast media are commonly used with CT to evaluate disease and to determine treatment response. The risk of acute kidney injury (AKI) developing in patients with reduced kidney function following exposure to intravenous iodinated contrast media has been overstated. This is due primarily to historic lack of control groups sufficient to separate contrast-induced AKI (CI-AKI; ie, AKI caused by contrast media administration) from contrast-associated AKI (CA-AKI; ie, AKI coincident to contrast media administration). Although the true risk of CI-AKI remains uncertain for patients with severe kidney disease, prophylaxis with intravenous normal saline is indicated for patients who have AKI or an estimated glomerular filtration rate less than 30 mL/min/1.73 m who are not undergoing maintenance dialysis. In individual high-risk circumstances, prophylaxis may be considered in patients with an estimated glomerular filtration rate of 30-44 mL/min/1.73 m at the discretion of the ordering clinician.
静脉注射碘化造影剂常用于CT检查,以评估疾病并确定治疗反应。肾功能减退患者在接触静脉注射碘化造影剂后发生急性肾损伤(AKI)的风险被高估了。这主要是由于以往缺乏足够的对照组来区分造影剂诱发的AKI(CI-AKI,即由造影剂给药引起的AKI)和造影剂相关的AKI(CA-AKI,即与造影剂给药同时发生的AKI)。虽然重度肾病患者发生CI-AKI的真实风险仍不确定,但对于未接受维持性透析且患有AKI或估计肾小球滤过率低于30 mL/min/1.73 m²的患者,建议静脉输注生理盐水进行预防。在个别高危情况下,经医嘱医生酌情考虑,估计肾小球滤过率为30-44 mL/min/1.73 m²的患者也可考虑进行预防。