Li Yong Sheng, Meng Fan Chun, Lin Jun Kai
Department of Colorectal surgery.
Department of Gastroenterology, Dongying Shengli Oilfield Central Hospital, Dongying, Shandong, P.R. China.
Medicine (Baltimore). 2020 Oct 2;99(40):e22431. doi: 10.1097/MD.0000000000022431.
In this analysis, we aimed to systematically compare the procedural and post-operative complications (POC) associated with laparoscopic versus open abdominal surgery for right-sided colonic cancer resection.
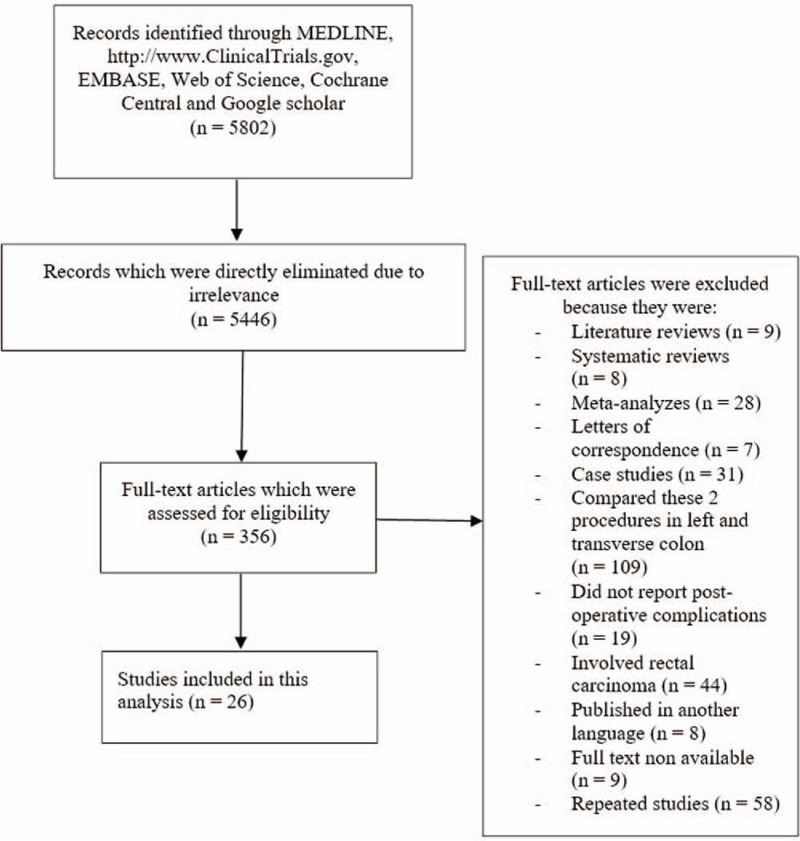
We searched MEDLINE, http://www.ClinicalTrials.gov, EMBASE, Web of Science, Cochrane Central, and Google scholar for English studies comparing the POC in patients who underwent laparoscopic versus open surgery (OS) for right colonic cancer. Data were assessed by the Cochrane-based RevMan 5.4 software (The Cochrane Community, London, UK). Mean difference (MD) with 95% confidence intervals (CIs) were used to represent the results for continuous variables, whereas risk ratios (RR) with 95% CIs were used for dichotomous data.
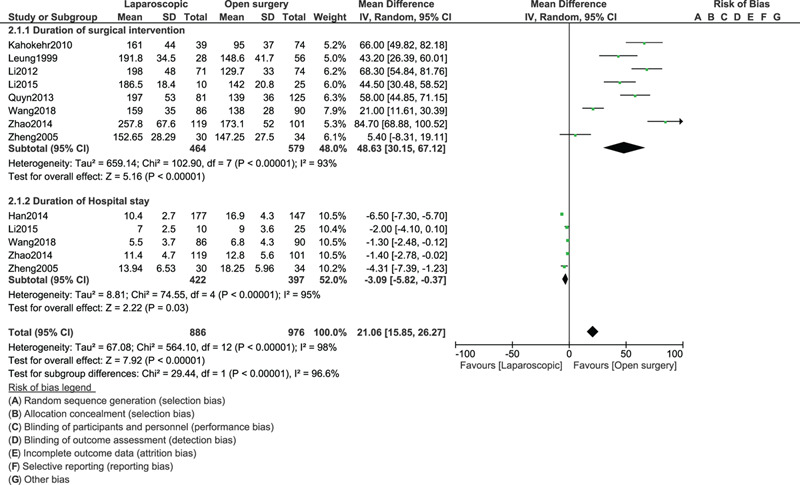
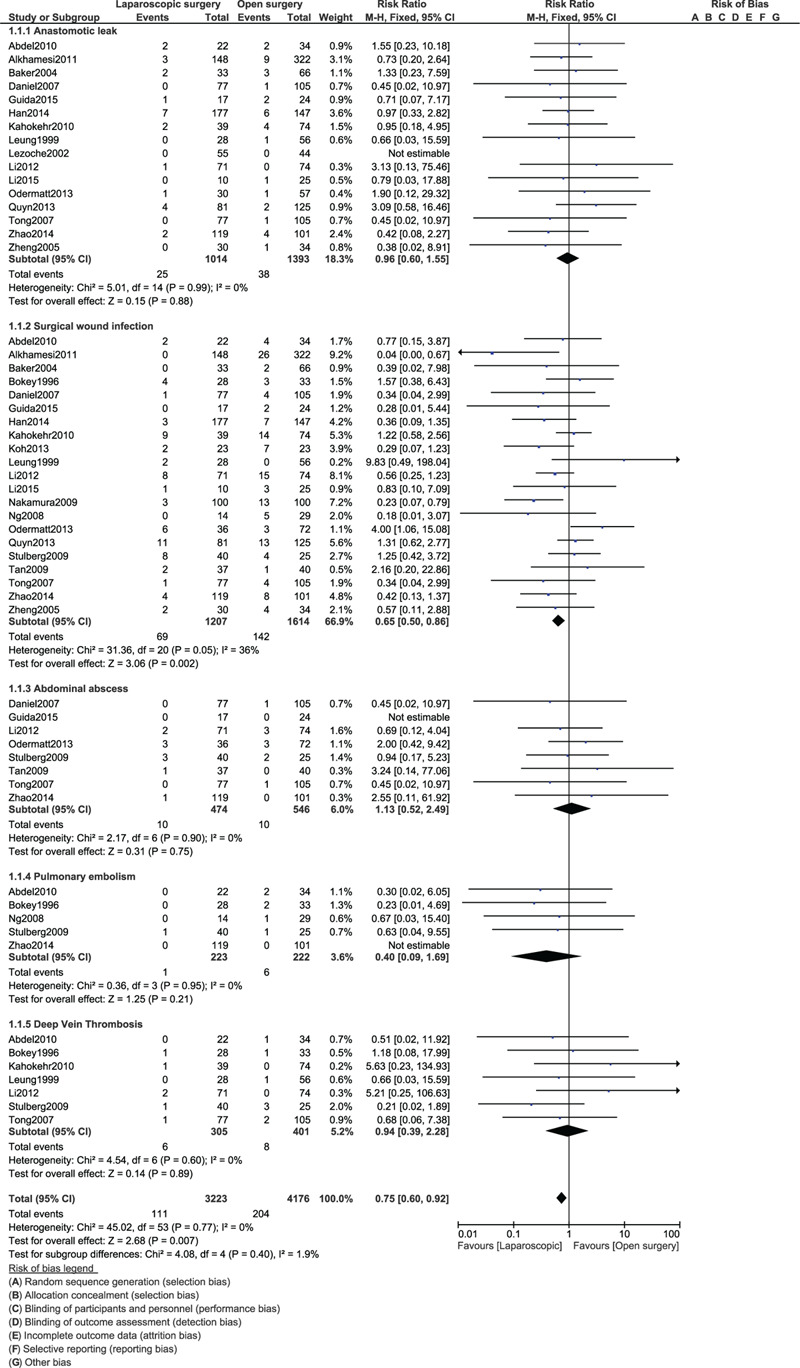
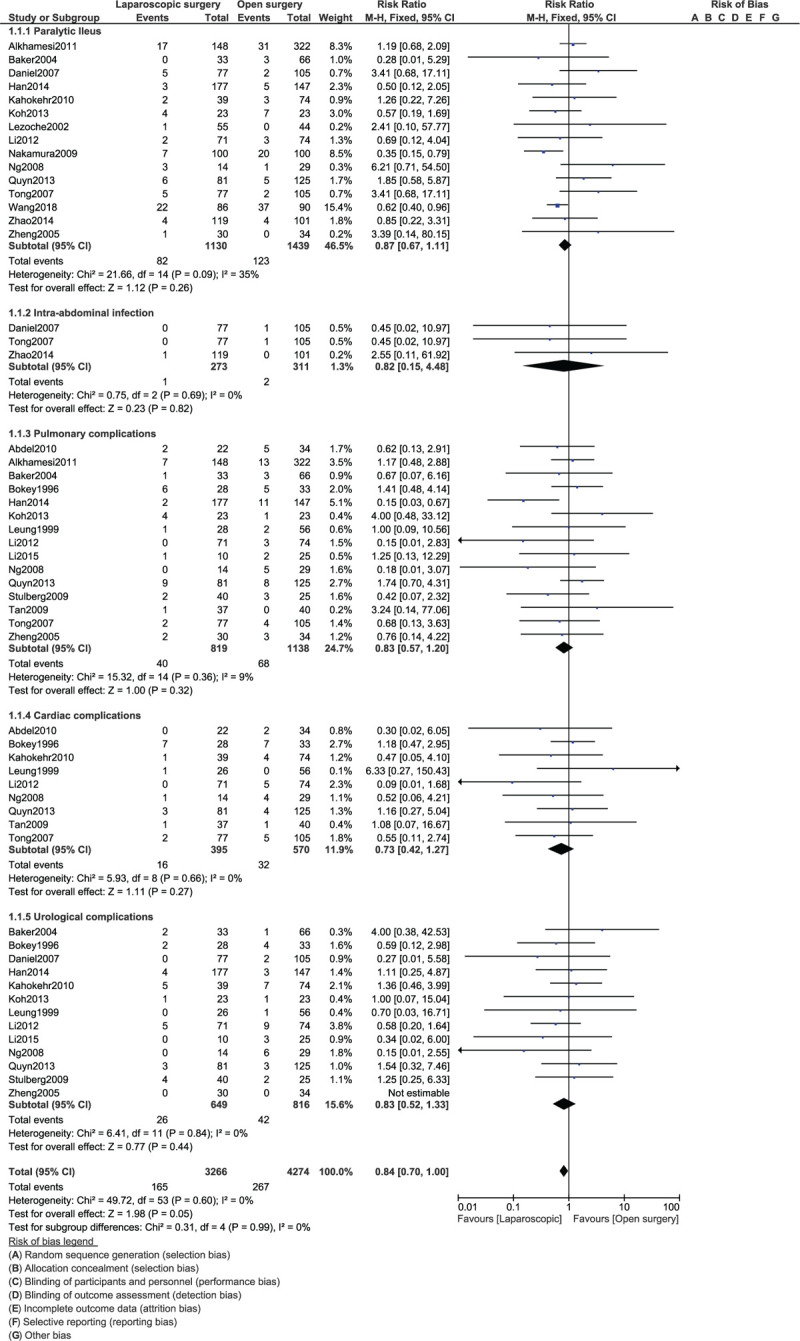
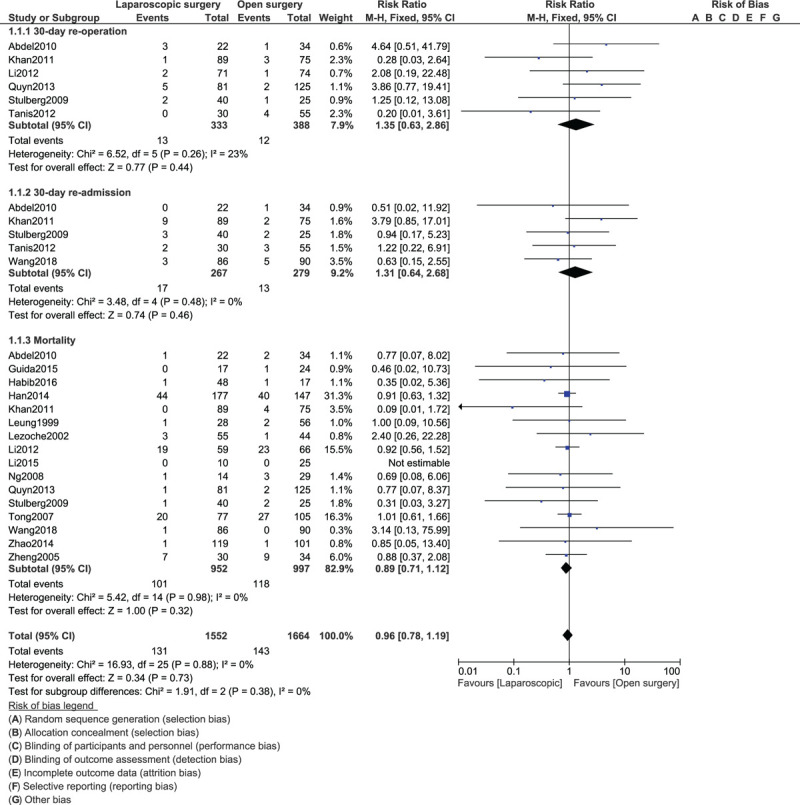
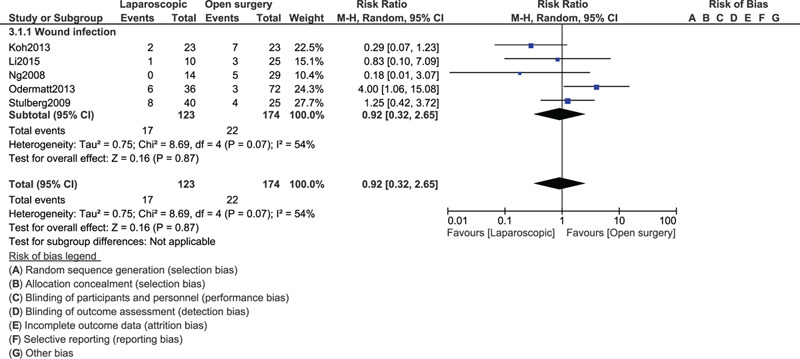
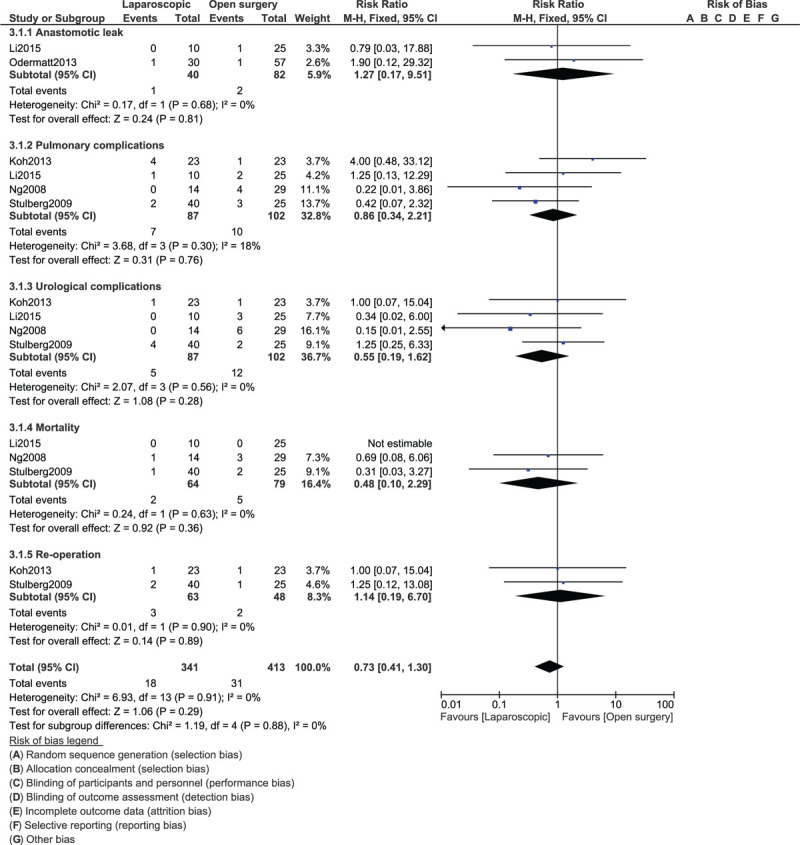
Twenty-six studies involving a total number of 3410 participants with right colonic carcinoma were included in this analysis. One thousand five hundred and fifteen participants were assigned to undergo invasive laparoscopic surgery whereas 1895 participants were assigned to the open abdominal surgery. Our results showed that the open resection was associated with a shorter length of surgery (MD: 48.63, 95% CI: 30.15-67.12; P = .00001) whereas laparoscopic intervention was associated with a shorter hospital stay [MD (-3.09), 95% CI [-5.82 to (-0.37)]; P = .03]. In addition, POC such as anastomotic leak (RR: 0.96, 95% CI: 0.60-1.55; P = .88), abdominal abscess (RR: 1.13, 95% CI: 0.52-2.49; P = .75), pulmonary embolism (RR: 0.40, 95% CI: 0.09-1.69; P = .21) and deep vein thrombosis (RR: 0.94, 95% CI: 0.39-2.28; P = .89) were not significantly different. Paralytic ileus (RR: 0.87, 95% CI: 0.67-1.11; P = .26), intra-abdominal infection (RR: 0.82, 95% CI: 0.15-4.48; P = .82), pulmonary complications (RR: 0.83, 95% CI: 0.57-1.20; P = .32), cardiac complications (RR: 0.73, 95% CI: 0.42-1.27; P = .27) and urological complications (RR: 0.83, 95% CI: 0.52-1.33; P = .44) were also similarly manifested. Our analysis also showed 30-day re-admission and re-operation, and mortality to be similar between laparoscopic versus OS for right colonic carcinoma resection. However, surgical wound infection (RR: 0.65, 95% CI: 0.50-0.86; P = .002) was significantly higher with the OS.
In conclusion, laparoscopic surgery was almost comparable to OS in terms of post-operative outcomes for right-sided colonic cancer resection and was not associated with higher unwanted outcomes. Therefore, laparoscopic intervention should be considered as safe as the open abdominal surgery for right-sided colonic cancer resection, with a decreased hospital stay.
在本分析中,我们旨在系统比较腹腔镜与开腹手术治疗右侧结肠癌切除术中的手术过程及术后并发症(POC)。
我们检索了MEDLINE、http://www.ClinicalTrials.gov、EMBASE、Web of Science、Cochrane Central和谷歌学术,以查找比较接受腹腔镜与开腹手术(OS)治疗右侧结肠癌患者POC的英文研究。数据采用基于Cochrane的RevMan 5.4软件(英国伦敦Cochrane协作网)进行评估。连续变量结果用95%置信区间(CI)的均值差(MD)表示,二分数据则用95%CI的风险比(RR)表示。
本分析纳入了26项研究,共3410例右侧结肠癌患者。1515例患者被分配接受侵入性腹腔镜手术,1895例患者被分配接受开腹手术。我们的结果显示,开腹切除术的手术时间较短(MD:48.63,95%CI:30.15 - 67.12;P = 0.00001),而腹腔镜干预的住院时间较短[MD(-3.09),95%CI[-5.82至(-0.37)];P = 0.03]。此外,诸如吻合口漏(RR:0.96,95%CI:0.60 - 1.55;P = 0.88)、腹腔脓肿(RR:1.13,95%CI:0.52 - 2.49;P = 0.75)、肺栓塞(RR:0.40,95%CI:0.09 - 1.69;P = 0.21)和深静脉血栓形成(RR:0.94,95%CI:0.39 - 2.28;P = 0.89)等POC无显著差异。麻痹性肠梗阻(RR:0.87,95%CI:0.67 - 1.11;P = 0.26)、腹腔内感染(RR:0.82,95%CI:0.15 - 4.48;P = 0.82)、肺部并发症(RR:0.83,95%CI:0.57 - 1.20;P = 0.32)、心脏并发症(RR:0.73,95%CI:0.42 - 1.27;P = 0.27)和泌尿系统并发症(RR:0.83,95%CI:0.52 - 1.33;P = 0.44)也表现相似。我们的分析还表明,右侧结肠癌切除术中腹腔镜手术与开腹手术在30天再入院、再次手术及死亡率方面相似。然而,开腹手术的手术伤口感染(RR:0.65,95%CI:0.50 - 0.86;P = 0.002)显著更高。
总之,在右侧结肠癌切除术后的结果方面,腹腔镜手术与开腹手术几乎相当,且不会导致更多不良后果。因此,对于右侧结肠癌切除术,腹腔镜干预应被视为与开腹手术一样安全,且住院时间更短。