Ha Ngoc Huong Lien, Chan Ivana, Yap Philip, Nurjono Milawaty, Vrijhoef Hubertus J M, Nicholas Sean Olivia, Wee Shiou-Liang
Geriatric Education and Research Institute, Singapore.
Department of Geriatric Medicine, Khoo Teck Puat Hospital, Singapore.
BMJ Open. 2020 Oct 5;10(10):e039017. doi: 10.1136/bmjopen-2020-039017.
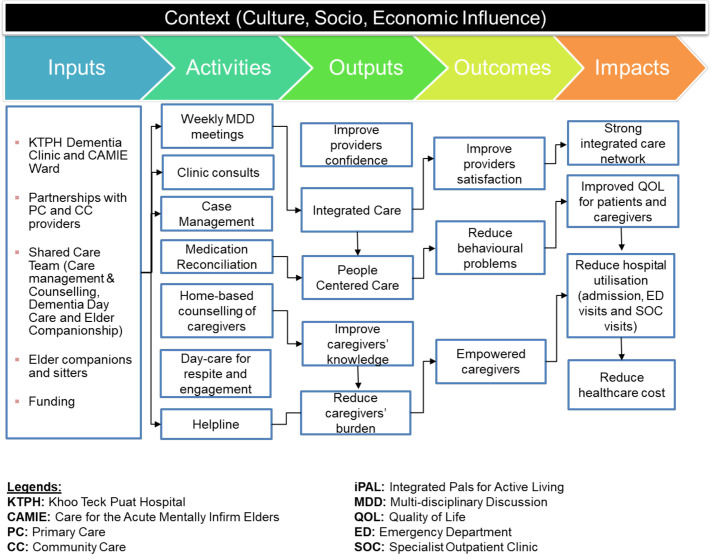
The capability and capacity of the primary and community care (PCC) sector for dementia in Singapore may be enhanced through better integration. Through a partnership involving a tertiary hospital and PCC providers, an integrated dementia care network (CARITAS: comprehensive, accessible, responsive, individualised, transdisciplinary, accountable and seamless) was implemented. The study evaluated the process and extent of integration within CARITAS.
Triangulation mixed-methods design and analyses were employed to understand factors underpinning network mechanisms.
The study was conducted at a tertiary hospital in the northern region of Singapore.
We recruited participants who were involved in the conceptualisation, design, development and implementation of the CARITAS Programme from a tertiary hospital and PCC providers.
We used the Rainbow Model of Integrated Care-Measurement Tool (RMIC-MT) to assess integration from managerial perspectives. RMIC-MT comprises eight dimensions that play interconnected roles on a macro-level, meso-level and microlevel. We administered RMIC-MT to healthcare providers and conducted in-depth interviews with key CARITAS stakeholders.
We assessed integration scores across eight dimensions of the RMIC-MT and factors underpinning network mechanisms.
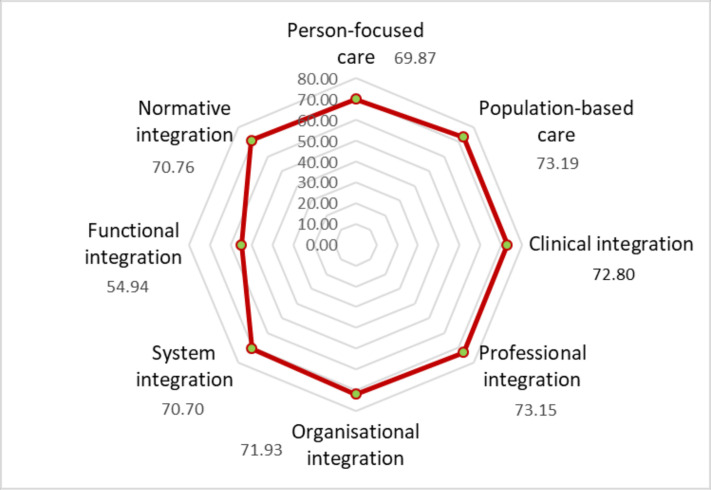
Compared with other dimensions, functional integration (mechanisms by which information and management modalities are linked) achieved the lowest mean score of 55. Other dimensions (eg, clinical, professional and organisational integration) scored about 70. Presence of inspiring clinical leaders and tacit interdependencies among partners strengthened the network. However, the lack of structured documentation and a shared information-technology platform hindered functional integration.
CARITAS has reached maturity in micro-levels and meso-levels of integration, while macro-integration needs further development. Integration can be enhanced by assessing service gaps, increasing engagement with stakeholders and providing a shared communication system.
通过更好的整合,可以提高新加坡基层和社区护理(PCC)部门应对痴呆症的能力。通过一家三级医院与PCC提供者的合作,实施了一个综合痴呆症护理网络(慈善关爱:全面、可及、响应性、个性化、跨学科、问责且无缝)。该研究评估了慈善关爱网络内整合的过程和程度。
采用三角混合方法设计和分析,以了解支撑网络机制的因素。
该研究在新加坡北部地区的一家三级医院进行。
我们从一家三级医院和PCC提供者中招募了参与慈善关爱项目概念化、设计、开发和实施的人员。
我们使用综合护理彩虹模型测量工具(RMIC-MT)从管理角度评估整合情况。RMIC-MT包括八个维度,这些维度在宏观、中观和微观层面发挥着相互关联的作用。我们对医疗保健提供者进行了RMIC-MT评估,并对慈善关爱项目的关键利益相关者进行了深入访谈。
我们评估了RMIC-MT八个维度的整合得分以及支撑网络机制的因素。
与其他维度相比,功能整合(信息和管理模式相联系的机制)的平均得分最低,为55分。其他维度(如临床、专业和组织整合)得分约为70分。有鼓舞人心的临床领导者以及合作伙伴之间的默契相互依存关系加强了网络。然而,缺乏结构化文档和共享信息技术平台阻碍了功能整合。
慈善关爱在微观和中观层面的整合已达到成熟水平,而宏观整合需要进一步发展。通过评估服务差距、增加与利益相关者的互动以及提供共享通信系统,可以加强整合。