Pillarisetti Ajay, Roy Sudipto, Diamond-Smith Nadia, Ghorpade Makarand, Dhongade Arun, Balakrishnan Kalpana, Sambandam Sankar, Patil Rutuja, Levine David I, Juvekar Sanjay, Smith Kirk R
Gangarosa Department of Environmental Health, Rollins School of Public Health, Atlanta, Georgia, USA
Vadu Rural Health Program, KEM Hospital Research Centre, Pune, India.
BMJ Open. 2020 Oct 5;10(10):e044127. doi: 10.1136/bmjopen-2020-044127.
Health interventions often target pregnant women and their unborn children. Interventions in rural India targeting pregnant women, however, often do not cover the critical early windows of susceptibility during the first trimester and parts of the second trimester. This pilot seeks to determine if targeting newlyweds could protect entire pregnancies with a clean stove and fuel intervention.
We recruited 50 newlywed couples who use biomass as a cooking fuel into a clean cooking intervention that included a liquefied petroleum gas (LPG) stove, two gas cylinders, a table to place the stove on and health education. We first evaluated whether community health workers in this region could identify and recruit couples at marriage. We quantified how many additional days of pregnancy could be covered by an intervention if we recruited at marriage versus recruiting after detection of pregnancy.
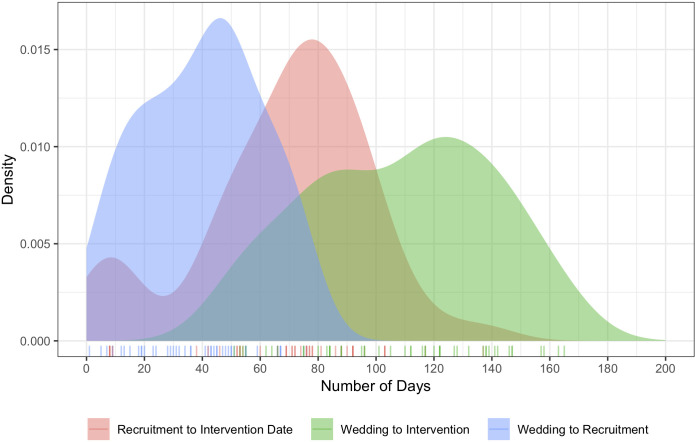
On average, we identified and visited newlywed couples within 40 (SD 21) days of marriage. Of the 50 couples recruited, 25 pregnancies and 18 deliveries were identified during this 1-year study. Due to challenges securing fuel from the LPG supply system, not all couples received their intervention prior to pregnancy. Regardless, couples recruited in the marriage arm had substantially more days with the intervention than couples recruited into a similar arm recruited at pregnancy (211 SD 46 vs 120 SD 45). At scale, a stove intervention targeting new marriages would cover about twice as many weeks of first pregnancies as an intervention recruiting after detection of pregnancy.
We were able to recruit in early marriage using existing community health workers. Households recruited early in marriage had more days with clean fuel coverage than those recruited at pregnancy. Our findings indicate that recruitment at marriage is feasible and warrants further exploration for stove and other interventions targeting pregnancy-related outcomes.
健康干预措施通常以孕妇及其未出生的孩子为目标。然而,印度农村地区针对孕妇的干预措施往往未能覆盖孕早期以及孕中期部分关键的易感染窗口期。本试点研究旨在确定针对新婚夫妇开展清洁炉灶和燃料干预措施是否能够保护整个孕期。
我们招募了50对使用生物质作为烹饪燃料的新婚夫妇,让他们参与一项清洁烹饪干预项目,该项目包括一个液化石油气(LPG)炉灶、两个气瓶、一张放置炉灶的桌子以及健康教育。我们首先评估了该地区的社区卫生工作者能否在新婚时识别并招募夫妇。我们量化了如果在新婚时招募与在检测到怀孕后招募相比,干预措施能够覆盖的额外孕期天数。
平均而言,我们在新婚夫妇结婚后40(标准差21)天内识别并走访了他们。在这项为期1年的研究中,招募的50对夫妇中有25例怀孕和18例分娩。由于从LPG供应系统获取燃料存在困难,并非所有夫妇在怀孕前都接受了干预措施。尽管如此,新婚时招募的夫妇接受干预的天数比怀孕时招募到类似组的夫妇多得多(211±46天对120±45天)。从规模上看,针对新婚夫妇的炉灶干预措施覆盖的首次怀孕周数大约是怀孕检测后招募的干预措施的两倍。
我们能够利用现有的社区卫生工作者在新婚早期进行招募。新婚早期招募的家庭使用清洁燃料的天数比怀孕时招募的家庭多。我们的研究结果表明,新婚时招募是可行的,值得进一步探索针对与怀孕相关结果的炉灶及其他干预措施。