Department of Clinical Neurosciences, Cambridge University, Cambridge, UK.
Harvard Medical School, Harvard University, Boston, Massachusetts, USA.
BMJ Open. 2020 Oct 5;10(10):e044566. doi: 10.1136/bmjopen-2020-044566.
To analyse enrolment to interventional trials during the first wave of the COVID-19 pandemic in England and describe the barriers to successful recruitment in the circumstance of a further wave or future pandemics.
We analysed registered interventional COVID-19 trial data and concurrently did a prospective observational study of hospitalised patients with COVID-19 who were being assessed for eligibility to one of the RECOVERY, C19-ACS or SIMPLE trials.
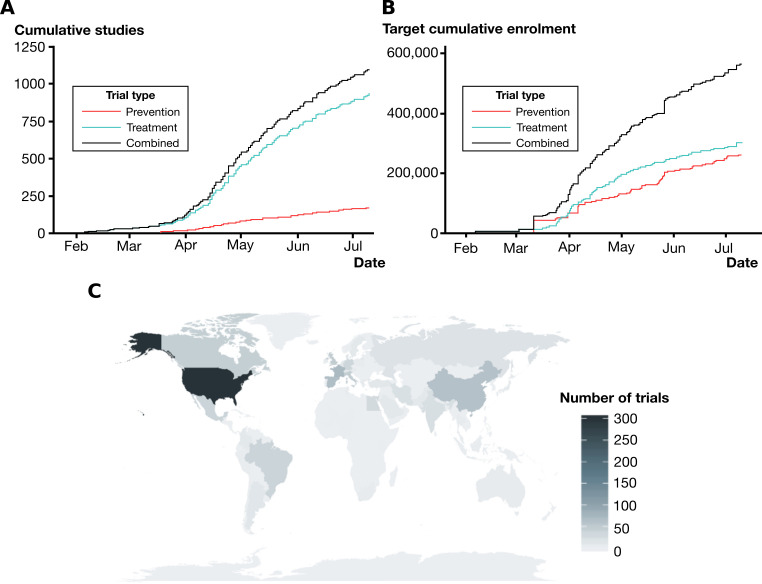
Interventional COVID-19 trial data were analysed from the clinicaltrials.gov and International Standard Randomized Controlled Trial Number databases on 12 July 2020. The patient cohort was taken from five centres in a respiratory National Institute for Health Research network. Population and modelling data were taken from published reports from the UK government and Medical Research Council Biostatistics Unit.
2082 consecutive admitted patients with laboratory-confirmed SARS-CoV-2 infection from 27 March 2020 were included.
Proportions enrolled, and reasons for exclusion from the aforementioned trials. Comparisons of trial recruitment targets with estimated feasible recruitment numbers.
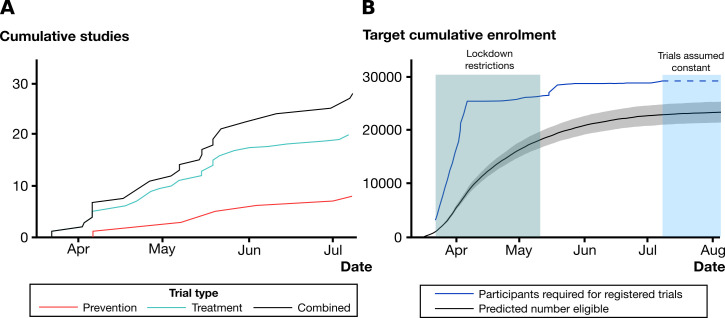
Analysis of trial registration data for COVID-19 treatment studies enrolling in England showed that by 12 July 2020, 29 142 participants were needed. In the observational study, 430 (20.7%) proceeded to randomisation. 82 (3.9%) declined participation, 699 (33.6%) were excluded on clinical grounds, 363 (17.4%) were medically fit for discharge and 153 (7.3%) were receiving palliative care. With 111 037 people hospitalised with COVID-19 in England by 12 July 2020, we determine that 22 985 people were potentially suitable for trial enrolment. We estimate a UK hospitalisation rate of 2.38%, and that another 1.25 million infections would be required to meet recruitment targets of ongoing trials.
Feasible recruitment rates, study design and proliferation of trials can limit the number, and size, that will successfully complete recruitment. We consider that fewer, more appropriately designed trials, prioritising cooperation between centres would maximise productivity in a further wave.
分析英格兰 COVID-19 大流行第一波期间介入性试验的入组情况,并描述在未来出现另一波或大流行时成功招募的障碍。
我们分析了已注册的 COVID-19 介入性试验数据,并同时对正在评估是否符合 RECOVERY、C19-ACS 或 SIMPLE 试验纳入标准的 COVID-19 住院患者进行了前瞻性观察性研究。
2020 年 7 月 12 日,我们从 clinicaltrials.gov 和国际标准随机对照试验编号数据库分析了 COVID-19 介入性试验数据。患者队列来自呼吸国立卫生研究院网络中的五个中心。人群和建模数据取自英国政府和医学研究理事会生物统计学部发布的报告。
纳入了 2020 年 3 月 27 日至 2020 年 3 月 27 日期间连续 27 名实验室确诊 SARS-CoV-2 感染的住院患者。
纳入比例以及排除上述试验的原因。试验招募目标与估计可行招募人数的比较。
对在英格兰招募 COVID-19 治疗研究的试验登记数据分析显示,截至 2020 年 7 月 12 日,需要招募 29142 名参与者。在观察性研究中,430 名(20.7%)患者接受了随机分组。82 名(3.9%)患者拒绝参与,699 名(33.6%)因临床原因被排除,363 名(17.4%)患者适合出院,153 名(7.3%)患者接受姑息治疗。根据 2020 年 7 月 12 日英格兰 COVID-19 住院患者人数,我们确定 22985 人可能适合参加试验。我们估计英国的住院率为 2.38%,要满足正在进行的试验的招募目标,还需要另外 125 万例感染。
可行的招募率、研究设计和试验的扩散可能会限制成功完成招募的人数和规模。我们认为,在未来的一波中,数量更少、设计更合理、优先考虑中心之间合作的试验将最大限度地提高生产力。