Hematology and Medical Oncology, Department of Clinical Therapeutics, National and Kapodistrian University of Athens, School of Medicine, Athens, Greece.
First Department of Medicine, Department of Hematology, First Faculty of Medicine, Charles University and General Hospital in Prague, Prague, Czech Republic.
J Clin Oncol. 2020 Dec 1;38(34):4030-4041. doi: 10.1200/JCO.20.02060. Epub 2020 Oct 6.
Maintenance therapy prolongs progression-free survival (PFS) in patients with newly diagnosed multiple myeloma (NDMM) not undergoing autologous stem cell transplantation (ASCT) but has generally been limited to immunomodulatory agents. Other options that complement the induction regimen with favorable toxicity are needed.
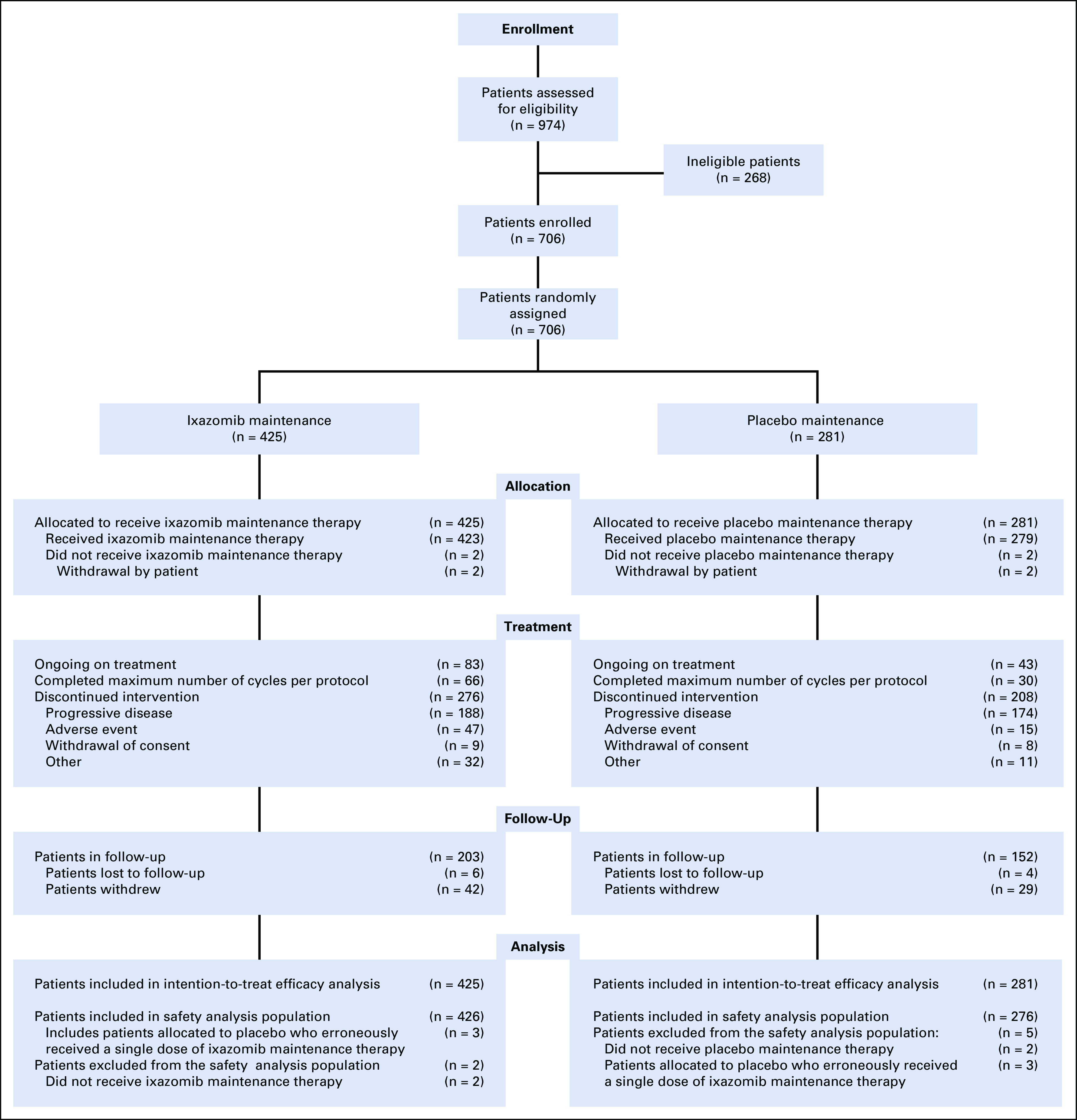
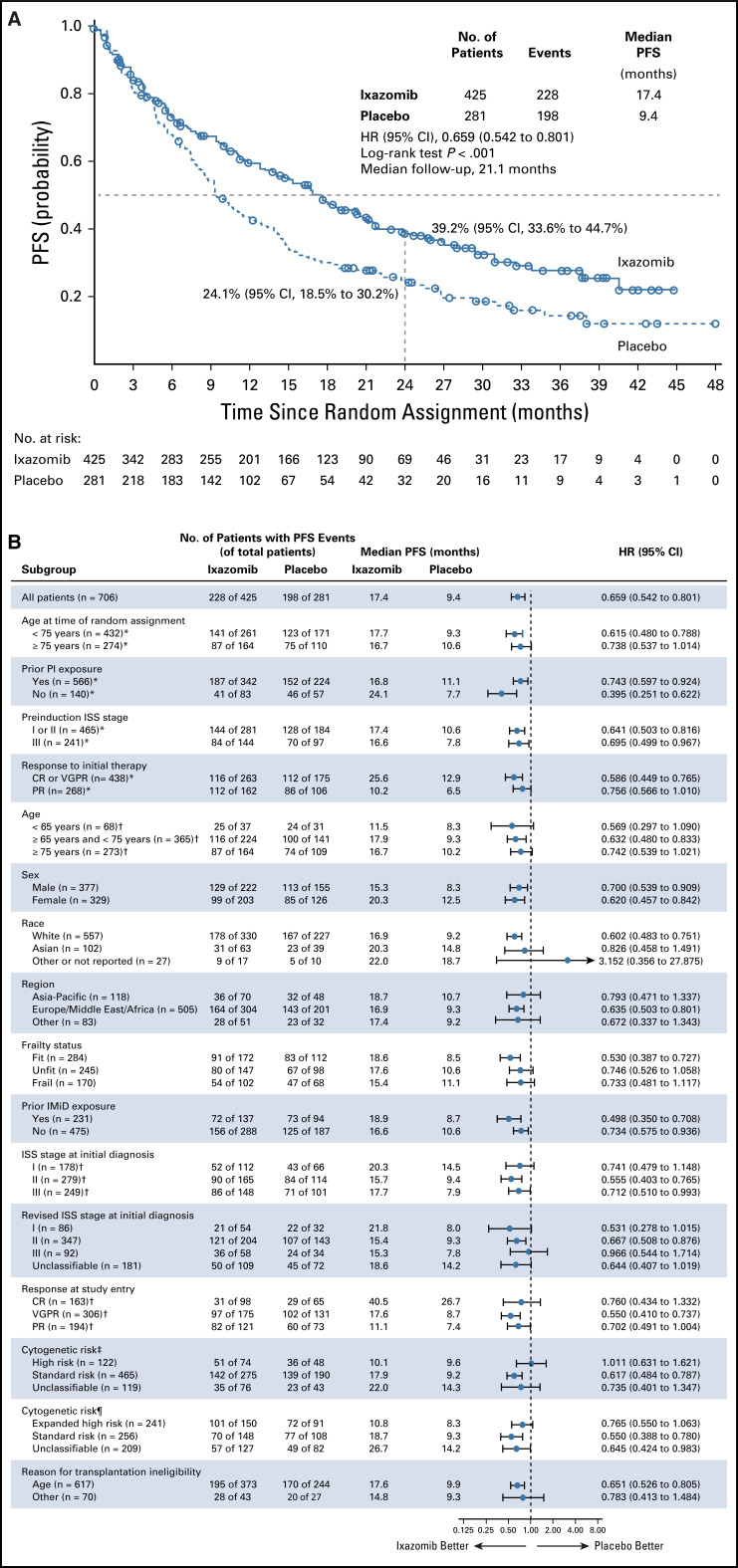
The phase III, double-blind, placebo-controlled TOURMALINE-MM4 study randomly assigned (3:2) patients with NDMM not undergoing ASCT who achieved better than or equal to partial response after 6-12 months of standard induction therapy to receive the oral proteasome inhibitor (PI) ixazomib or placebo on days 1, 8, and 15 of 28-day cycles as maintenance for 24 months. The primary endpoint was PFS since time of randomization.
Patients were randomly assigned to receive ixazomib (n = 425) or placebo (n = 281). TOURMALINE-MM4 met its primary endpoint with a 34.1% reduction in risk of progression or death with ixazomib versus placebo (median PFS since randomization, 17.4 9.4 months; hazard ratio [HR], 0.659; 95% CI, 0.542 to 0.801; < .001; median follow-up, 21.1 months). Ixazomib significantly benefitted patients who achieved complete or very good partial response postinduction (median PFS, 25.6 12.9 months; HR, 0.586; < .001). With ixazomib versus placebo, 36.6% versus 23.2% of patients had grade ≥ 3 treatment-emergent adverse events (TEAEs); 12.9% versus 8.0% discontinued treatment because of TEAEs. Common any-grade TEAEs included nausea (26.8% 8.0%), vomiting (24.2% 4.3%), and diarrhea (23.2% 12.3%). There was no increase in new primary malignancies (5.2% 6.2%); rates of on-study deaths were 2.6% versus 2.2%.
Ixazomib maintenance prolongs PFS with no unexpected toxicity in patients with NDMM not undergoing ASCT. To our knowledge, this is the first PI demonstrated in a randomized clinical trial to have single-agent efficacy for maintenance and is the first oral PI option in this patient population.
在未接受自体干细胞移植(ASCT)的新诊断多发性骨髓瘤(NDMM)患者中,维持治疗可延长无进展生存期(PFS),但通常仅限于免疫调节药物。需要其他补充诱导方案且毒性良好的选择。
III 期、双盲、安慰剂对照的 TOURMALINE-MM4 研究将未接受 ASCT、在标准诱导治疗 6-12 个月后获得优于或等于部分缓解的 NDMM 患者随机(3:2)分配,接受口服蛋白酶体抑制剂(PI)伊沙佐米或安慰剂,在 28 天周期的第 1、8 和 15 天接受维持治疗 24 个月。主要终点是自随机分组以来的 PFS。
患者被随机分配接受伊沙佐米(n = 425)或安慰剂(n = 281)。TOURMALINE-MM4 达到了主要终点,与安慰剂相比,伊沙佐米降低了 34.1%的进展或死亡风险(自随机分组以来的中位 PFS,17.4 9.4 个月;风险比[HR],0.659;95%CI,0.542 至 0.801;<0.001;中位随访时间,21.1 个月)。伊沙佐米使诱导后获得完全或非常好的部分缓解的患者显著受益(中位 PFS,25.6 12.9 个月;HR,0.586;<0.001)。与安慰剂相比,36.6%的患者与 23.2%的患者发生≥3 级治疗相关不良事件(TEAEs);12.9%与 8.0%的患者因 TEAEs 停药。常见的任何级别 TEAEs 包括恶心(26.8% 8.0%)、呕吐(24.2% 4.3%)和腹泻(23.2% 12.3%)。未增加新发原发性恶性肿瘤(5.2% 6.2%);研究期间的死亡率为 2.6%与 2.2%。
伊沙佐米维持治疗可延长未接受 ASCT 的 NDMM 患者的 PFS,且无意外毒性。据我们所知,这是第一项在随机临床试验中证明单药维持治疗有效的 PI,也是该患者人群中第一种口服 PI 选择。