Department of Internal Medicine, Brigham & Women's Hospital, Boston, Massachusetts.
Division of Population Sciences, Dana-Farber Cancer Institute, Boston, Massachusetts.
JAMA Netw Open. 2024 Jun 3;7(6):e2414425. doi: 10.1001/jamanetworkopen.2024.14425.
Published research suggests that patient-reported outcomes (PROs) are neither commonly collected nor reported in randomized clinical trials (RCTs) for solid tumors. Little is known about these practices in RCTs for hematological malignant neoplasms.
To evaluate the prevalence of PROs as prespecified end points in RCTs of hematological malignant neoplasms, and to assess reporting of PROs in associated trial publications.
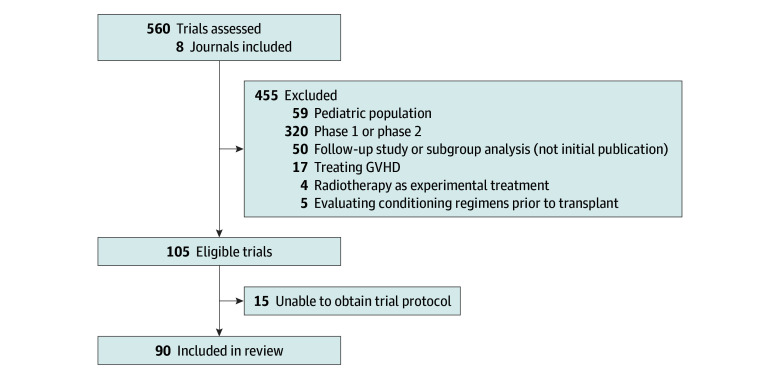
All issues of 8 journals known for publishing high-impact RCTs (NEJM, Lancet, Lancet Hematology, Lancet Oncology, Journal of Clinical Oncology, Blood, JAMA, and JAMA Oncology) between January 1, 2018, and December 13, 2022, were searched for primary publications of therapeutic phase 3 trials for adults with hematological malignant neoplasms. Studies that evaluated pretransplant conditioning regimens, graft-vs-host disease treatment, or radiotherapy as experimental treatment were excluded. Data regarding trial characteristics and PROs were extracted from manuscripts and trial protocols. Univariable analyses assessed associations between trial characteristics and PRO collection or reporting.
Ninety RCTs were eligible for analysis. PROs were an end point in 66 (73%) trials: in 1 trial (1%) as a primary end point, in 50 (56%) as a secondary end point, and in 15 (17%) as an exploratory end point. PRO data were reported in 26 of 66 primary publications (39%): outcomes were unchanged in 18 and improved in 8, with none reporting worse PROs with experimental treatment. Trials sponsored by for-profit entities were more likely to include PROs as an end point (49 of 55 [89%] vs 17 of 35 [49%]; P < .001) but were not significantly more likely to report PRO data (20 of 49 [41%] vs 6 of 17 [35%]; P = .69). Compared with trials involving lymphoma (18 of 29 [62%]) or leukemia or myelodysplastic syndrome (18 of 28 [64%]), those involving plasma cell disorders or multiple myeloma (27 of 30 [90%]) or myeloproliferative neoplasms (3 of 3 [100%]) were more likely to include PROs as an end point (P = .03). Similarly, compared with trials involving lymphoma (3 of 18 [17%]) or leukemia or myelodysplastic syndrome (5 of 18 [28%]), those involving plasma cell disorders or multiple myeloma (16 of 27 [59%]) or myeloproliferative neoplasms (2 of 3 [67%]) were more likely to report PROs in the primary publication (P = .01).
In this systematic review, almost 3 of every 4 therapeutic RCTs for blood cancers collected PRO data; however, only 1 RCT included PROs as a primary end point. Moreover, most did not report resulting PRO data in the primary publication and when reported, PROs were either better or unchanged, raising concern for publication bias. This analysis suggests a critical gap in dissemination of data on the lived experiences of patients enrolled in RCTs for hematological malignant neoplasms.
已发表的研究表明,在实体瘤的随机临床试验(RCT)中,患者报告的结局(PROs)既不常见也未报告。关于血液恶性肿瘤的 RCT 中这些实践的了解甚少。
评估血液恶性肿瘤的 RCT 中 PRO 作为预设终点的流行程度,并评估相关试验出版物中 PRO 的报告情况。
检索了 8 种知名期刊的所有问题,这些期刊在发表高影响力 RCT 方面表现出色(《新英格兰医学杂志》、《柳叶刀》、《柳叶刀血液学》、《柳叶刀肿瘤学》、《临床肿瘤学杂志》、《血液》、《美国医学会杂志》和《美国医学会肿瘤学杂志》),时间范围为 2018 年 1 月 1 日至 2022 年 12 月 13 日,内容为成人血液恶性肿瘤的治疗性 3 期试验的主要出版物。评估移植前预处理方案、移植物抗宿主病治疗或放疗作为实验治疗的研究被排除在外。从手稿和试验方案中提取有关试验特征和 PRO 的数据。单变量分析评估了试验特征与 PRO 收集或报告之间的关联。
90 项 RCT 符合分析条件。66 项试验(73%)将 PRO 作为终点:1 项试验(1%)作为主要终点,50 项(56%)作为次要终点,15 项(17%)作为探索性终点。66 项主要出版物中有 26 项(39%)报告了 PRO 数据:18 项无变化,8 项改善,没有一项报告实验治疗的 PRO 更差。由营利性实体赞助的试验更有可能将 PRO 作为终点(55 项中的 49 项[89%]与 35 项中的 17 项[49%];P<0.001),但报告 PRO 数据的可能性并不显著更高(49 项中的 20 项[41%]与 17 项中的 6 项[35%];P=0.69)。与涉及淋巴瘤(29 项中的 18 项[62%])或白血病或骨髓增生异常综合征(28 项中的 18 项[64%])的试验相比,涉及浆细胞疾病或多发性骨髓瘤(30 项中的 27 项[90%])或骨髓增生性肿瘤(3 项中的 3 项[100%])的试验更有可能将 PRO 作为终点(P=0.03)。同样,与涉及淋巴瘤(18 项中的 3 项[17%])或白血病或骨髓增生异常综合征(18 项中的 5 项[28%])的试验相比,涉及浆细胞疾病或多发性骨髓瘤(27 项中的 16 项[59%])或骨髓增生性肿瘤(3 项中的 2 项[67%])的试验更有可能在主要出版物中报告 PRO(P=0.01)。
在这项系统评价中,近 3/4 的血液癌症治疗性 RCT 收集了 PRO 数据;然而,只有 1 项 RCT 将 PRO 作为主要终点。此外,大多数试验未在主要出版物中报告由此产生的 PRO 数据,而且当报告时,PRO 要么更好,要么不变,这引发了对发表偏倚的担忧。这项分析表明,在血液恶性肿瘤的 RCT 中,患者生存体验的数据传播存在重大差距。