Division of Paediatric Critical Care Medicine, Department of Paediatrics, Beatrix Children's Hospital, University Medical Center Groningen, The University of Groningen, Internal Postal Code CA 80, P.O. Box 30.001, 9700, RB, Groningen, the Netherlands.
Critical Care, Anesthesia, Peri-operative Medicine & Emergency Medicine (CAPE), The University of Groningen, Groningen, the Netherlands.
Crit Care. 2020 Oct 7;24(1):601. doi: 10.1186/s13054-020-03313-7.
Recurrent delivery of tidal mechanical energy (ME) inflicts ventilator-induced lung injury (VILI) when stress and strain exceed the limits of tissue tolerance. Mechanical power (MP) is the mathematical description of the ME delivered to the respiratory system over time. It is unknown how ME relates to underlying lung pathology and outcome in mechanically ventilated children. We therefore tested the hypothesis that ME per breath with tidal volume (Vt) normalized to bodyweight correlates with underlying lung pathology and to study the effect of resistance on the ME dissipated to the lung.
We analyzed routinely collected demographic, physiological, and laboratory data from deeply sedated and/or paralyzed children < 18 years with and without lung injury. Patients were stratified into respiratory system mechanic subgroups according to the Pediatric Mechanical Ventilation Consensus Conference (PEMVECC) definition. The association between MP, ME, lung pathology, and duration of mechanical ventilation as a primary outcome measure was analyzed adjusting for confounding variables and effect modifiers. The effect of endotracheal tube diameter (ETT) and airway resistance on energy dissipation to the lung was analyzed in a bench model with different lung compliance settings.
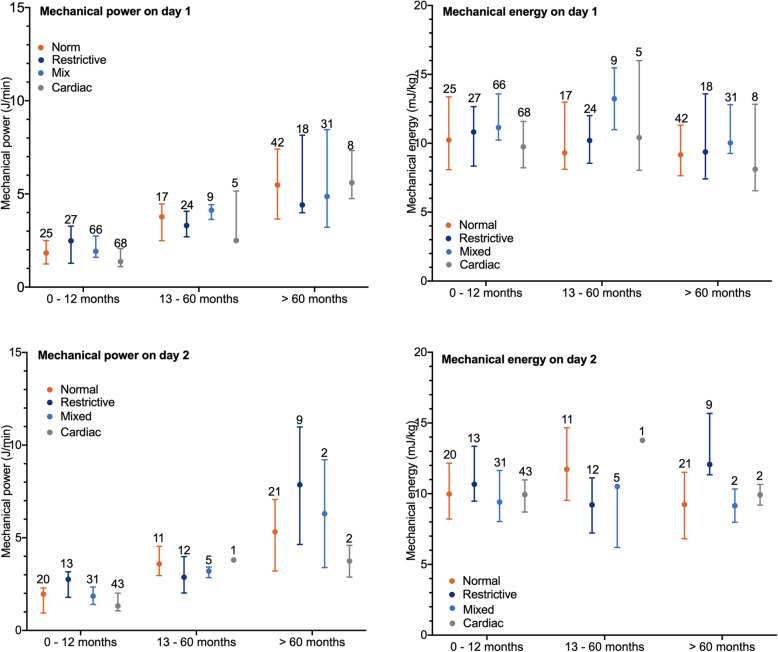
Data of 312 patients with a median age of 7.8 (1.7-44.2) months was analyzed. Age (p < 0.001), RR p < 0.001), and Vt < 0.001) were independently associated with MPrs. ME but not MP correlated significantly (p < 0.001) better with lung pathology. Competing risk regression analysis adjusting for PRISM III 24 h score and PEMVECC stratification showed that ME on day 1 or day 2 of MV but not MP was independently associated with the duration of mechanical ventilation. About 33% of all energy generated by the ventilator was transferred to the lung and highly dependent on lung compliance and airway resistance but not on endotracheal tube size (ETT) during pressure control (PC) ventilation.
ME better related to underlying lung pathology and patient outcome than MP. The delivery of generated energy to the lung was not dependent on ETT size during PC ventilation. Further studies are needed to identify injurious MErs thresholds in ventilated children.
当应力和应变超过组织耐受极限时,反复传递潮汐机械能(ME)会导致呼吸机引起的肺损伤(VILI)。机械功率(MP)是随时间传递到呼吸系统的 ME 的数学描述。尚不清楚 ME 与机械通气儿童的潜在肺病理学和结果有何关系。因此,我们假设潮气量(Vt)标准化至体重的每呼吸 ME 与潜在的肺病理学相关,并研究阻力对传递到肺的 ME 的耗散的影响。
我们分析了镇静和/或麻痹的<18 岁患有和不患有肺损伤的儿童的常规收集的人口统计学、生理学和实验室数据。根据小儿机械通气共识会议(PEMVECC)的定义,将患者分为呼吸系统力学亚组。分析调整混杂变量和效应修饰剂后,MP、ME、肺病理学和机械通气时间作为主要结局指标之间的相关性。在不同肺顺应性设置的台式模型中分析了气管内管直径(ETT)和气道阻力对能量向肺耗散的影响。
共分析了 312 名中位年龄为 7.8(1.7-44.2)个月的患者的数据。年龄(p<0.001)、RR(p<0.001)和 Vt(p<0.001)与 MPrs 独立相关。ME 与机械通气时间显著相关(p<0.001),但与 MP 相关性更好。调整 PRISM III 24 小时评分和 PEMVECC 分层后,竞争风险回归分析显示,机械通气第 1 天或第 2 天的 ME 而不是 MP 与机械通气时间独立相关。在压力控制(PC)通气期间,呼吸机产生的所有能量约有 33%转移到肺部,并且高度依赖于肺顺应性和气道阻力,而与气管内管大小(ETT)无关。
ME 与潜在的肺病理学和患者预后的相关性优于 MP。在 PC 通气期间,向肺部输送产生的能量不依赖于 ETT 大小。需要进一步研究以确定机械通气儿童的致伤 ME 阈值。