Vollmert Thomas, Hellmich Martin, Gassanov Natig, Er Fikret, Yücel Seyrani, Erdmann Erland, Caglayan Evren
Department III for Internal Medicine, University of Cologne, Cologne, Germany.
Institute of Medical Statistics and Computational Biology (IMSB), Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany.
Eur J Med Res. 2020 Oct 8;25(1):47. doi: 10.1186/s40001-020-00448-9.
Heart failure is a syndrome with increasing prevalence in concordance with the aging population and better survival rates from myocardial infarction. Morbidity and mortality are high in chronic heart failure patients, particularly in those with hospital admission for acute decompensation. Several risk stratification tools and score systems have been established to predict mortality in chronic heart failure patients. However, identification of patients at risk with easy obtainable clinical factors that can predict mortality in acute decompensated heart failure (ADHF) are needed to optimize the care-path.
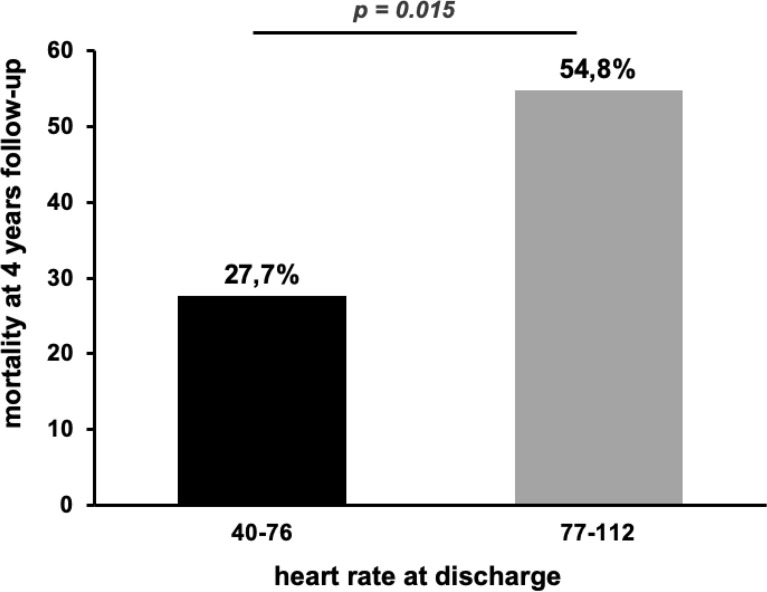
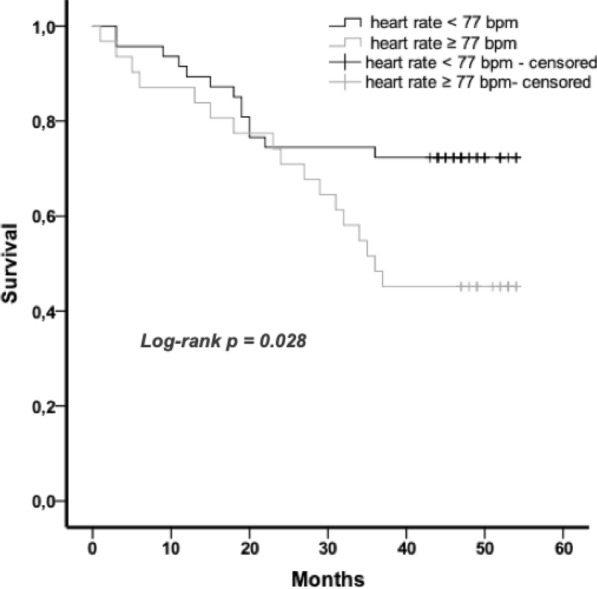
We retrospectively analyzed electronic medical records of 78 patients with HFrEF and HFmrEF who were hospitalized with ADHF in the Heart Center of the University Hospital Cologne in the year 2011 and discharged from the ward after successful treatment. 37.6 ± 16.4 months after index hospitalization 30 (38.5%) patients had died. This mortality rate correlated well with the calculated predicted survival with the Seattle Heart Failure Model (SHFM) for each individual patient. In our cohort, we identified elevated heart rate at discharge as an independent predictor for mortality (p = 0.016). The mean heart rate at discharge was lower in survived patients compared to patients who died (72.5 ± 11.9 vs. 79.1 ± 11.2 bpm. Heart rate of 77 bpm or higher was associated with an almost doubled mortality risk (p = 0.015). Heart rate elevation of 5 bpm was associated with an increase of mortality of 25% (p = 0.022).
Patients hospitalized for ADHF seem to have a better prognosis, when heart rate at discharge is < 77 bpm. Heart rate at discharge is an easily obtainable biomarker for risk prediction of mortality in HFrEF and HFmrEF patients treated for acute cardiac decompensation. Taking into account this parameter could be useful for guiding treatment strategies in these high-risk patients. Prospective data for validation of this biomarker and specific intervention are needed.
心力衰竭是一种随着人口老龄化和心肌梗死生存率提高而患病率不断上升的综合征。慢性心力衰竭患者的发病率和死亡率很高,尤其是那些因急性失代偿而住院的患者。已经建立了几种风险分层工具和评分系统来预测慢性心力衰竭患者的死亡率。然而,需要通过易于获得的临床因素识别有风险的患者,这些因素能够预测急性失代偿性心力衰竭(ADHF)的死亡率,以优化治疗路径。
我们回顾性分析了2011年在科隆大学医院心脏中心因ADHF住院并在成功治疗后从病房出院的78例射血分数降低的心力衰竭(HFrEF)和射血分数中间值的心力衰竭(HFmrEF)患者的电子病历。在首次住院后37.6±16.4个月,30例(38.5%)患者死亡。该死亡率与使用西雅图心力衰竭模型(SHFM)为每位患者计算的预测生存率密切相关。在我们的队列中,我们确定出院时心率升高是死亡率的独立预测因素(p=0.016)。存活患者出院时的平均心率低于死亡患者(72.5±11.9对79.1±11.2次/分)。心率达到或高于77次/分与死亡风险几乎翻倍相关(p=0.015)。心率升高5次/分与死亡率增加25%相关(p=0.022)。
因ADHF住院的患者出院时心率<77次/分时,预后似乎更好。出院时心率是HFrEF和HFmrEF患者急性心脏失代偿治疗中死亡率风险预测的易于获得的生物标志物。考虑到这一参数可能有助于指导这些高危患者的治疗策略。需要前瞻性数据来验证这一生物标志物并进行特异性干预。