Department of Cardiology, Tokyo Women's Medical University, 8-1 Kawada-cho, Shinjuku-ku, Tokyo, 162-8666, Japan.
Department of Cardiology, Tokyo Women's Medical University Yachiyo Medical Center, Yachiyo, Japan.
ESC Heart Fail. 2019 Jun;6(3):475-486. doi: 10.1002/ehf2.12418. Epub 2019 Mar 3.
There are regional differences in the patient characteristics, management, and outcomes of hospitalized patients with heart failure (HF). The aim of this study was to evaluate the clinical characteristics and outcomes of Japanese patients who are hospitalized with HF on the basis of the left ventricular ejection fraction (LVEF) stratum.
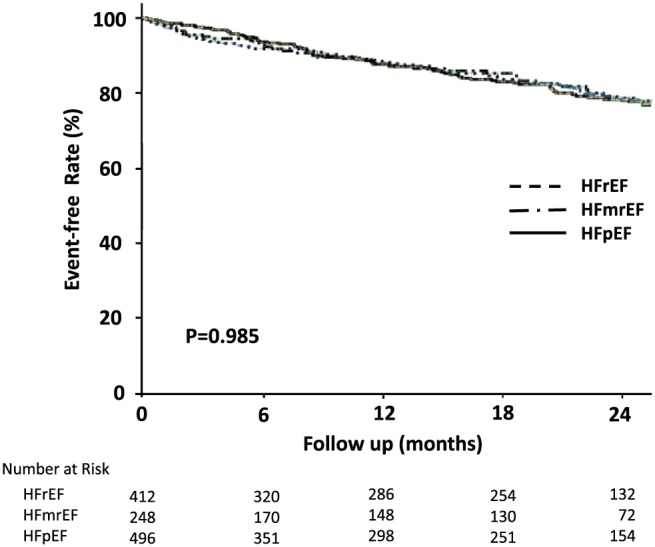
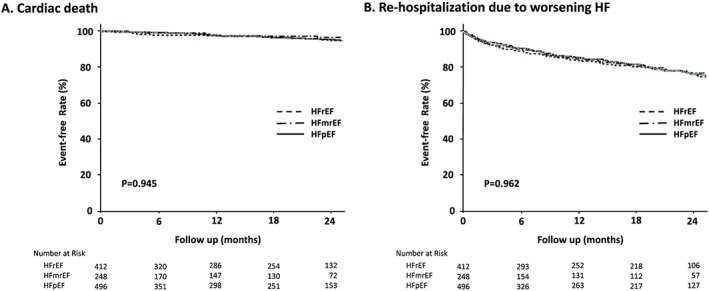
We retrospectively conducted a multicentre cohort study of 1245 hospitalized patients with decompensated HF between 2013 and 2014. Of these patients, 36% had an LVEF < 40% [HF with reduced ejection fraction (HFrEF), median age 72 years, 71% male], 21% had an LVEF 40-49% [HF with mid-range EF (HFmrEF), 77 years, 56% male], and 43% had an LVEF ≥ 50% [HF with preserved EF (HFpEF), 81 years, 44% male]. The primary outcome was death from any cause, and the secondary outcomes were cardiac death and re-hospitalization due to worsened HF after hospital discharge. There were high proportions of non-ischaemic cardiomyopathy (32%) in HFrEF patients, coronary artery disease (44%) in HFmrEF patients, and valvular disease (39%) in HFpEF patients. The frequencies of intravenous diuretic and natriuretic peptide administration during hospitalization were 66% and 30%, respectively. The median hospital stay for the overall population was 19 days, and the length of stay was >7 days for >90% of patients. In-hospital mortality was 7%, but was not different among the LVEF groups (HFrEF 7%, HFmrEF 6%, and HFpEF 8%). After a median follow-up of 19 months (range, 3-26 months), 192 (17%) of the 1156 patients who were discharged alive died, and 534 (46%) were re-hospitalized after hospital discharge. There were no significant differences in mortality after hospital discharge among the three LVEF groups (HFrEF 18%, HFmrEF 16%, and HFpEF 16%). There were no differences in cardiac death or re-hospitalization due to worsened HF after hospital discharge among the LVEF groups (cardiac death: HFrEF 8%, HFmrEF 7%, and HFpEF 7%; re-hospitalization due to worsened HF: HFrEF 19%, HFmrEF 16%, and HFpEF 17%). Multivariable-adjusted analyses showed that the HFmrEF and HFrEF groups, compared with the HFpEF group, were not associated with an increased risk for in-hospital death or death after hospital discharge. Non-cardiac causes of death and re-hospitalization after hospital discharge accounted for 35% and 38%, respectively.
Our results revealed different clinical characteristics but similar mortality rates in the HFrEF, HFmrEF, and HFpEF groups. The most common cause of death and re-hospitalization after hospital discharge was HF, but non-cardiac causes also contributed to their prognosis. Integrated management approaches will be required for HF patients.
心力衰竭(HF)住院患者的患者特征、治疗和结局存在地域差异。本研究旨在根据左心室射血分数(LVEF)分层评估日本 HF 住院患者的临床特征和结局。
我们回顾性地对 2013 年至 2014 年期间 1245 例失代偿性 HF 住院患者进行了一项多中心队列研究。这些患者中,36%的 LVEF<40%[射血分数降低的心力衰竭(HFrEF),中位年龄 72 岁,71%为男性],21%的 LVEF 为 40-49%[HF 射血分数中间范围(HFmrEF),77 岁,56%为男性],43%的 LVEF≥50%[HF 射血分数保留(HFpEF),81 岁,44%为男性]。主要结局是任何原因导致的死亡,次要结局是心脏死亡和出院后因 HF 恶化而再住院。HFrEF 患者中非缺血性心肌病(32%)、HFmrEF 患者中冠状动脉疾病(44%)和 HFpEF 患者中瓣膜疾病(39%)的比例较高。住院期间静脉利尿剂和利钠肽的使用频率分别为 66%和 30%。总体人群的中位住院时间为 19 天,>90%的患者住院时间>7 天。院内死亡率为 7%,但在 LVEF 组之间无差异(HFrEF 7%,HFmrEF 6%,HFpEF 8%)。中位随访 19 个月(范围,3-26 个月)后,1156 例出院存活患者中有 192 例(17%)死亡,534 例(46%)出院后再住院。出院后死亡率在 LVEF 三组之间无显著差异(HFrEF 18%,HFmrEF 16%,HFpEF 16%)。出院后心脏死亡或因 HF 恶化再住院在 LVEF 组之间无差异(心脏死亡:HFrEF 8%,HFmrEF 7%,HFpEF 7%;因 HF 恶化再住院:HFrEF 19%,HFmrEF 16%,HFpEF 17%)。多变量调整分析显示,HFmrEF 和 HFrEF 组与 HFpEF 组相比,院内死亡或出院后死亡的风险无增加。非心脏原因死亡和出院后再住院分别占 35%和 38%。
我们的研究结果表明,HFrEF、HFmrEF 和 HFpEF 三组患者的临床特征不同,但死亡率相似。HF 是导致死亡和出院后再住院的最常见原因,但非心脏原因也会影响预后。需要对 HF 患者采取综合管理方法。