Harrington Heart and Vascular Institute, University Hospitals, Cleveland, OH, USA.
Kent State University, College of Public Health, Kent, OH, USA.
J Cardiovasc Magn Reson. 2020 Oct 12;22(1):74. doi: 10.1186/s12968-020-00664-6.
Human Immunodeficiency Virus (HIV) patients commonly experience dyspnea for which an immediate cause may not be always apparent. In this prospective cohort study of HIV patients with exercise limitation, we use cardiopulmonary exercise testing (CPET) coupled with exercise cardiovascular magnetic resonance (CMR) to elucidate etiologies of dyspnea.
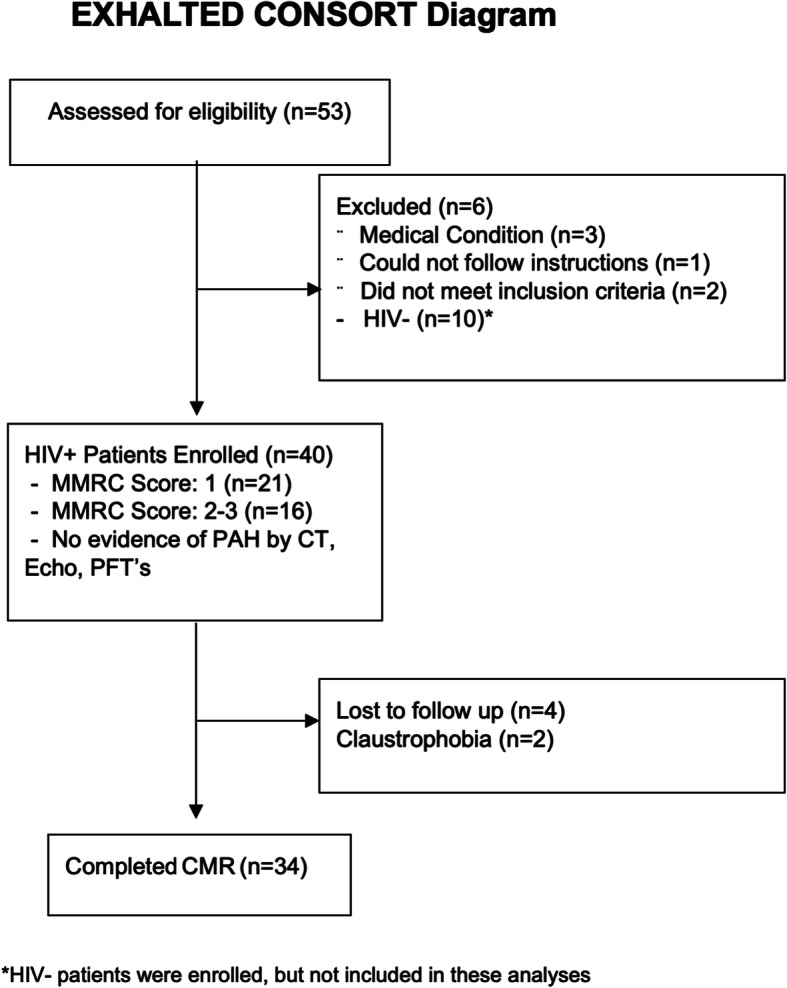
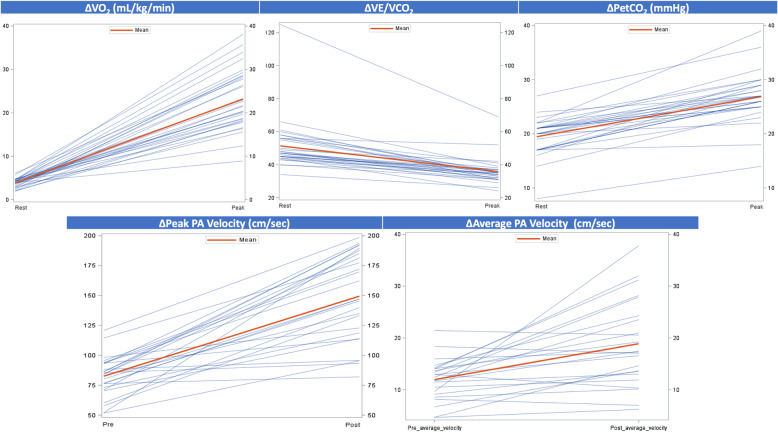
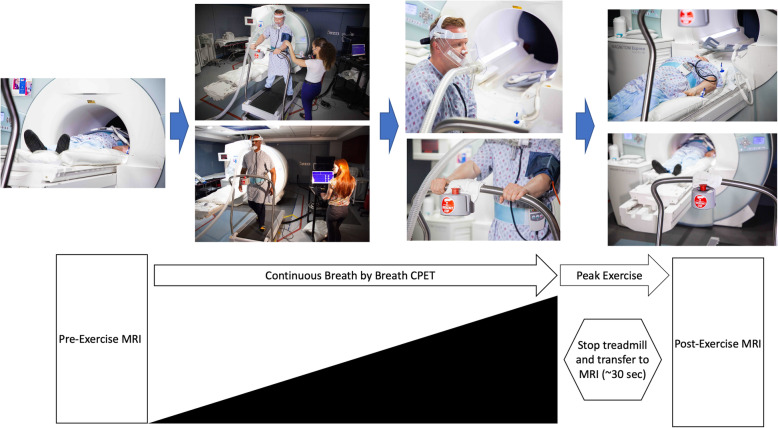
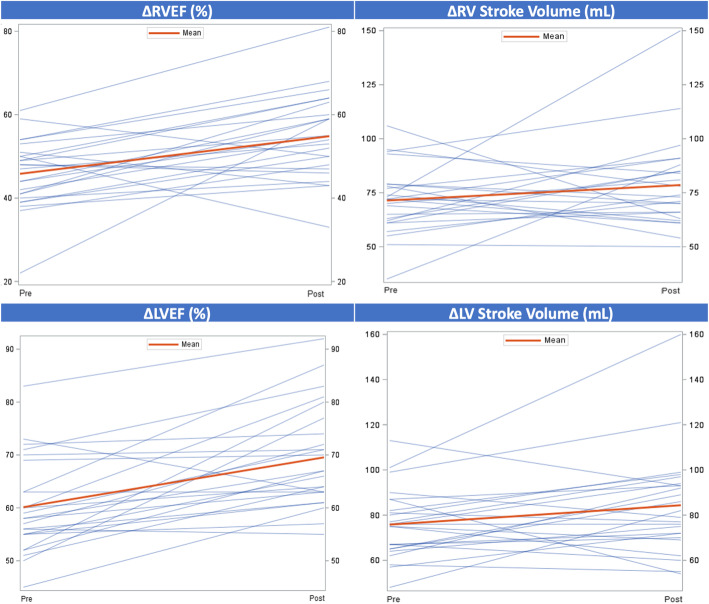
Thirty-four HIV patients on antiretroviral therapy with dyspnea and exercise limitation (49.7 years, 65% male, mean absolute CD4 count 700) underwent comprehensive evaluation with combined rest and maximal exercise treadmill CMR and CPET. The overall mean oxygen consumption (VO) peak was reduced at 23.2 ± 6.9 ml/kg/min with 20 patients (58.8% of overall cohort) achieving a respiratory exchange ratio > 1. The ventilatory efficiency (VE)/VCO slope was elevated at 36 ± 7.92, while ventilatory reserve (VE: maximal voluntary ventilation (MVV)) was within normal limits. The mean absolute right ventricular (RV) and left ventricular (LV) contractile reserves were preserved at 9.0% ± 11.2 and 9.4% ± 9.4, respectively. The average resting and post-exercise mean average pulmonary artery velocities were 12.2 ± 3.9 cm/s and 18.9 ± 8.3 respectively, which suggested lack of exercise induced pulmonary artery hypertension (PAH). LV but not RV delayed enhancement were identified in five patients. Correlation analysis found no relationship between peak VO measures of contractile RV or LV reserve, but LV and RV stroke volume correlated with PET CO (p = 0.02, p = 0.03).
Well treated patients with HIV appear to have conserved RV and LV function, contractile reserve and no evidence of exercise induced PAH. However, we found evidence of impaired ventilation suggesting a non-cardiopulmonary etiology for dyspnea.
人类免疫缺陷病毒(HIV)患者常出现呼吸困难,但通常无法明确其即时病因。在这项针对运动受限的 HIV 患者的前瞻性队列研究中,我们使用心肺运动测试(CPET)结合运动心血管磁共振(CMR)来阐明呼吸困难的病因。
34 名接受抗逆转录病毒治疗的 HIV 患者出现呼吸困难和运动受限(49.7 岁,65%为男性,平均绝对 CD4 计数为 700),接受了综合评估,包括静息和最大运动跑步机 CMR 和 CPET。整体平均摄氧量(VO)峰值为 23.2±6.9ml/kg/min,20 名患者(总队列的 58.8%)达到呼吸交换比>1。通气效率(VE)/VCO 斜率升高至 36±7.92,而通气储备(VE:最大自主通气量(MVV))处于正常范围内。平均绝对右心室(RV)和左心室(LV)收缩储备分别为 9.0%±11.2%和 9.4%±9.4%。平均静息和运动后平均肺动脉速度分别为 12.2±3.9cm/s 和 18.9±8.3cm/s,提示无运动诱导性肺动脉高压(PAH)。5 名患者发现 LV 但不是 RV 延迟增强。相关性分析发现,收缩储备的 RV 或 LV 峰值 VO 测量值之间没有关系,但 LV 和 RV 心搏量与 PET CO 相关(p=0.02,p=0.03)。
经过良好治疗的 HIV 患者似乎具有保留的 RV 和 LV 功能、收缩储备,并且没有运动诱导性 PAH 的证据。然而,我们发现通气受损的证据,这表明呼吸困难的非心肺病因。