Thokala Praveen, Stevenson Matt, Kumar Varun M, Ren Shijie, Ellis Alexandra G, Chapman Richard H
School of Health and Related Research, University of Sheffield, Sheffield, UK.
Previously At Institute for Clinical and Economic Review (ICER), Boston, MA USA.
Cost Eff Resour Alloc. 2020 Oct 6;18:41. doi: 10.1186/s12962-020-00234-8. eCollection 2020.
Patients with infantile-onset spinal muscular atrophy (SMA), a rare, genetic neuromuscular disease, do not achieve key motor function milestones (e.g., sitting) and have short life expectancy in the absence of treatment. Nusinersen is a disease-modifying therapy for patients with SMA.
The aim of this study was to estimate the cost-effectiveness of nusinersen compared to best supportive care (BSC) in patients diagnosed with infantile-onset SMA in the US.
A de novo economic model was developed with the following health states: "permanent ventilation", "not sitting", "sitting", "walking", and "death". Short-term data were sourced from the pivotal clinical trials and studies of nusinersen (ENDEAR and SHINE). Motor function milestones achieved at the end of follow-up in the clinical trials were assumed to be sustained until death. Mortality risks were based on survival modelling of relevant published Kaplan-Meier data. Costs, life years (LYs), and quality-adjusted life years (QALYs) were discounted at 3% per annum, and the analyses were performed from a US health care sector perspective. Scenario analyses and sensitivity analyses were conducted to assess the robustness of the results to key parameters.
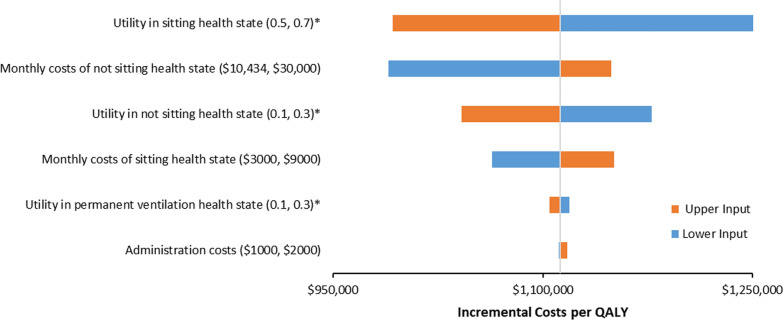
In our base-case analysis, nusinersen treatment achieves greater QALYs and more LYs (3.24 and 7.64, respectively) compared with BSC (0.46 QALYs and 2.40 LYs, respectively), resulting in an incremental cost per QALY gained of approximately $1,112,000 and an incremental cost per LY gained of $590,000 for nusinersen compared to BSC. The incremental cost effectiveness ratios did not fall below $990,000 per QALY gained in scenario and sensitivity analyses. Results were most sensitive to the length of survival, background health care costs, and utility in the "not sitting" and "sitting" health states.
The estimated incremental cost-effectiveness of nusinersen from a US health care sector perspective exceeded traditional cost-effectiveness thresholds. Cost-effectiveness was dependent on assumptions made regarding survival, costs, utilities, and whether the motor function milestones were sustained over lifetime. Given the relatively short-term effectiveness data available for the treatment, a registry to collect long-term data of infantile-onset SMA patients is recommended.
婴儿型脊髓性肌萎缩症(SMA)是一种罕见的遗传性神经肌肉疾病,患者在未接受治疗的情况下无法达到关键运动功能里程碑(如坐立),且预期寿命较短。诺西那生钠是一种用于治疗SMA患者的疾病修正疗法。
本研究旨在评估在美国,与最佳支持治疗(BSC)相比,诺西那生钠的成本效益。
建立了一个全新的经济模型,包含以下健康状态:“永久通气”“无法坐立”“能坐立”“能行走”和“死亡”。短期数据来源于诺西那生钠的关键临床试验和研究(ENDEAR和SHINE)。假设临床试验随访结束时达到的运动功能里程碑会持续至死亡。死亡风险基于相关已发表的Kaplan-Meier数据的生存模型。成本、生命年(LYs)和质量调整生命年(QALYs)按每年3%进行贴现,分析从美国医疗保健部门的角度进行。进行了情景分析和敏感性分析,以评估结果对关键参数的稳健性。
在我们的基础案例分析中,与BSC(分别为0.46个QALY和2.40个LY)相比,诺西那生钠治疗可实现更多的QALY和LY(分别为3.24和7.64),与BSC相比,诺西那生钠每获得一个QALY的增量成本约为111.2万美元,每获得一个LY的增量成本为59万美元。在情景分析和敏感性分析中,增量成本效益比未降至每获得一个QALY低于99万美元。结果对生存时长、背景医疗保健成本以及“无法坐立”和“能坐立”健康状态下的效用最为敏感。
从美国医疗保健部门的角度估计,诺西那生钠的增量成本效益超过了传统成本效益阈值。成本效益取决于关于生存、成本、效用以及运动功能里程碑是否能终身持续的假设。鉴于该治疗可用的短期有效性数据,建议建立一个登记系统来收集婴儿型SMA患者的长期数据。