Department of Radiation Oncology, Henry Ford Health System, Detroit, MI, USA.
Department of Radiation Oncology, Washington University, St. Louis, MO, USA.
J Appl Clin Med Phys. 2020 Nov;21(11):288-294. doi: 10.1002/acm2.13041. Epub 2020 Oct 12.
To investigate the differences between internal target volumes (ITVs) contoured on the simulation 4DCT and daily 4DCBCT images for lung cancer patients treated with stereotactic body radiotherapy (SBRT) and determine the dose delivered on 4D planning technique.
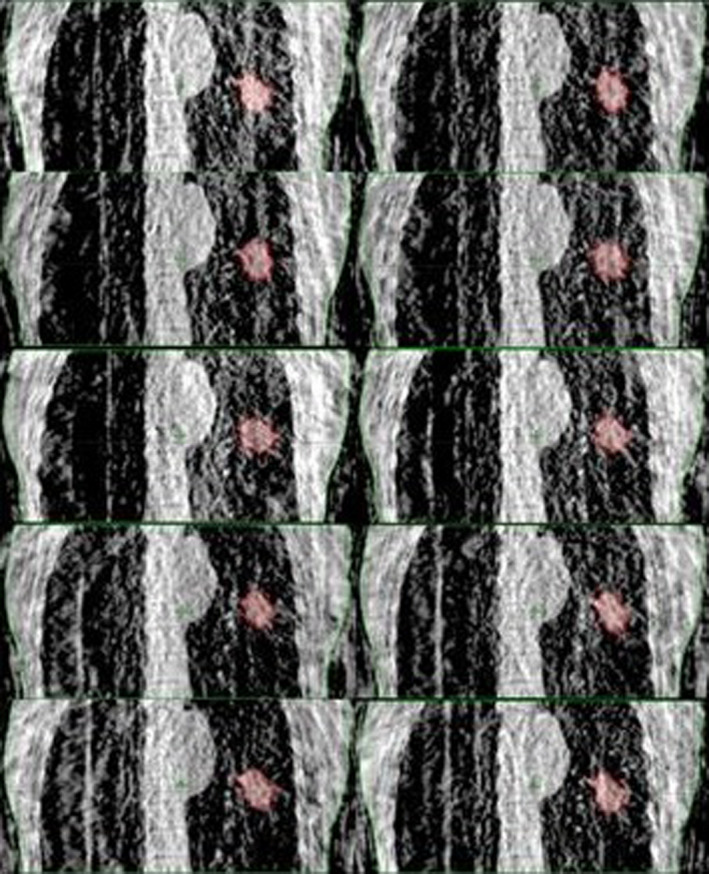
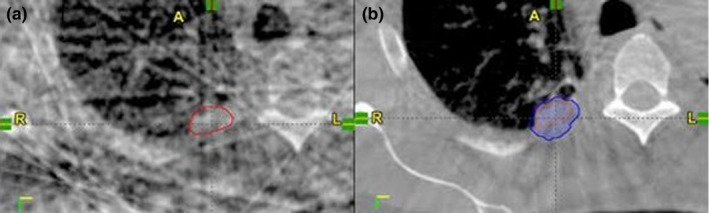
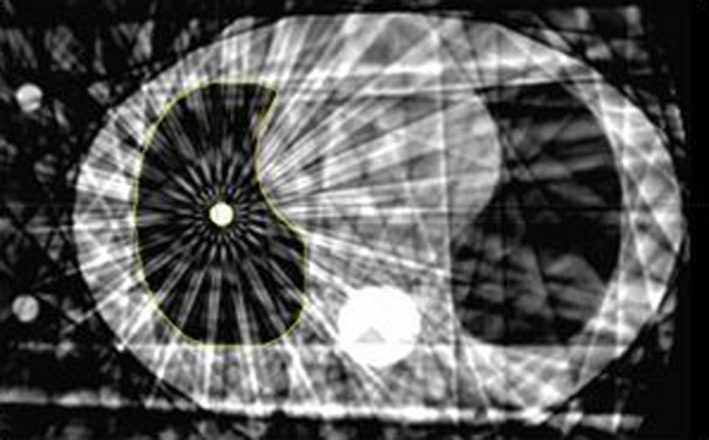
For nine patients, 4DCBCTs were acquired before each fraction to assess tumor motion. An ITV was contoured on each phase of the 4DCBCT and a union of the 10 ITVs was used to create a composite ITV. Another ITV was drawn on the average 3DCBCT (avgCBCT) to compare with current clinical practice. The Dice coefficient, Hausdorff distance, and center of mass (COM) were averaged over four fractions to compare the ITVs contoured on the 4DCT, avgCBCT, and 4DCBCT for each patient. Planning was done on the average CT, and using the online registration, plans were calculated on each phase of the 4DCBCT and on the avgCBCT. Plan dose calculations were tested by measuring ion chamber dose in the CIRS lung phantom.
The Dice coefficients were similar for all three comparisons: avgCBCT-to-4DCBCT (0.7 ± 0.1), 4DCT-to-avgCBCT (0.7 ± 0.1), and 4DCT-to-4DCBCT (0.7 ± 0.1); while the mean COM differences were also comparable (2.6 ± 2.2mm, 2.3 ± 1.4mm, and 3.1 ± 1.1mm, respectively). The Hausdorff distances for the comparisons with 4DCBCT (8.2 ± 2.9mm and 8.1 ± 3.2mm) were larger than the comparison without (6.5 ± 2.5mm). The differences in ITV D95% between the treatment plan and avgCBCT calculations were 4.3 ± 3.0% and -0.5 ± 4.6%, between treatment plan and 4DCBCT plans, respectively, while the ITV V100% coverages were 99.0 ± 1.9% and 93.1 ± 8.0% for avgCBCT and 4DCBCT, respectively.
There is great potential for 4DCBCT to evaluate the extent of tumor motion before treatment, but image quality challenges the clinician to consistently delineate lung target volumes.
研究立体定向体部放疗(SBRT)治疗肺癌患者时,在模拟 4DCT 上勾画的内部靶区(ITV)与每日 4D 锥形束 CT(4DCBCT)图像之间的差异,并确定 4D 计划技术的剂量分布。
对 9 例患者,在每次分割治疗前进行 4DCBCT 采集以评估肿瘤运动。在 4DCBCT 的每个时相上勾画 ITV,并对 10 个 ITV 进行并集以创建一个复合 ITV。在平均 3D 锥形束 CT(avgCBCT)上勾画另一个 ITV,与当前的临床实践进行比较。将 4 个分割的 ITV 勾画结果的 Dice 系数、Hausdorff 距离和质心(COM)进行平均,以比较每位患者在 4DCT、avgCBCT 和 4DCBCT 上勾画的 ITV。在平均 CT 上进行计划,并通过在线配准,在 4DCBCT 的每个时相和 avgCBCT 上计算计划。在 CIRS 肺部体模中测量离子室剂量来测试计划剂量计算。
所有三种比较的 Dice 系数都相似:avgCBCT 与 4DCBCT(0.7±0.1)、4DCT 与 avgCBCT(0.7±0.1)和 4DCT 与 4DCBCT(0.7±0.1);而平均 COM 差异也相当(分别为 2.6±2.2mm、2.3±1.4mm 和 3.1±1.1mm)。与 4DCBCT 比较的 Hausdorff 距离(8.2±2.9mm 和 8.1±3.2mm)大于无 4DCBCT 比较(6.5±2.5mm)。治疗计划与 avgCBCT 计算的 ITV D95%差异分别为 4.3±3.0%和-0.5±4.6%,而 ITV V100%覆盖度分别为 99.0±1.9%和 93.1±8.0%,用于 avgCBCT 和 4DCBCT。
4DCBCT 具有评估治疗前肿瘤运动范围的巨大潜力,但图像质量挑战临床医生始终如一地勾画肺部靶区。