Department of Obstetrics and Gynaecology, University of Cambridge, NIHR Cambridge Comprehensive Biomedical Research Centre, Cambridge, United Kingdom.
Birmingham Clinical Trials Unit, University of Birmingham, Birmingham, United Kingdom.
PLoS Med. 2020 Oct 13;17(10):e1003190. doi: 10.1371/journal.pmed.1003190. eCollection 2020 Oct.
The effectiveness of screening for macrosomia is not well established. One of the critical elements of an effective screening program is the diagnostic accuracy of a test at predicting the condition. The objective of this study is to investigate the diagnostic effectiveness of universal ultrasonic fetal biometry in predicting the delivery of a macrosomic infant, shoulder dystocia, and associated neonatal morbidity in low- and mixed-risk populations.
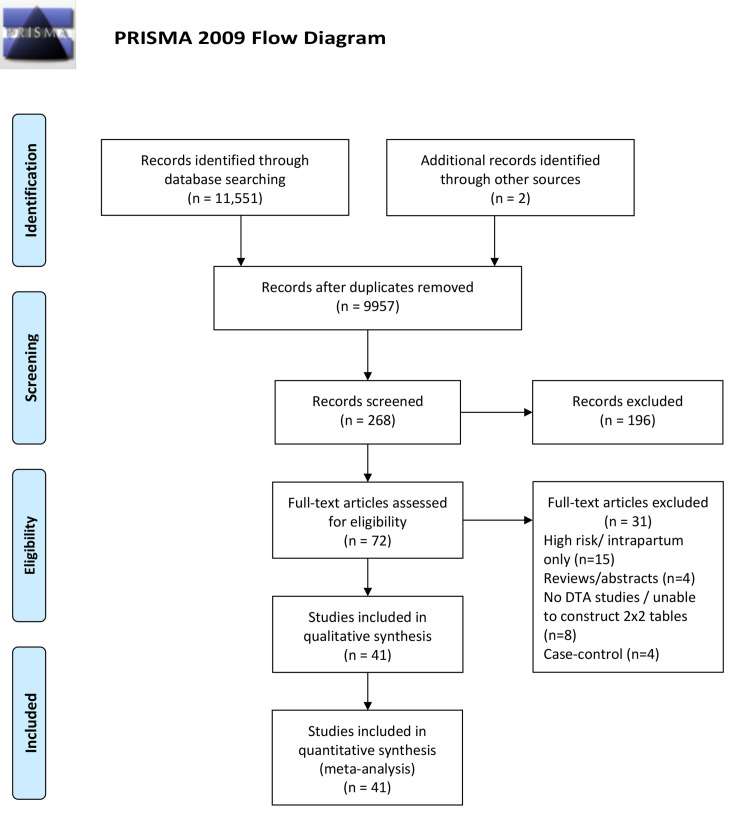
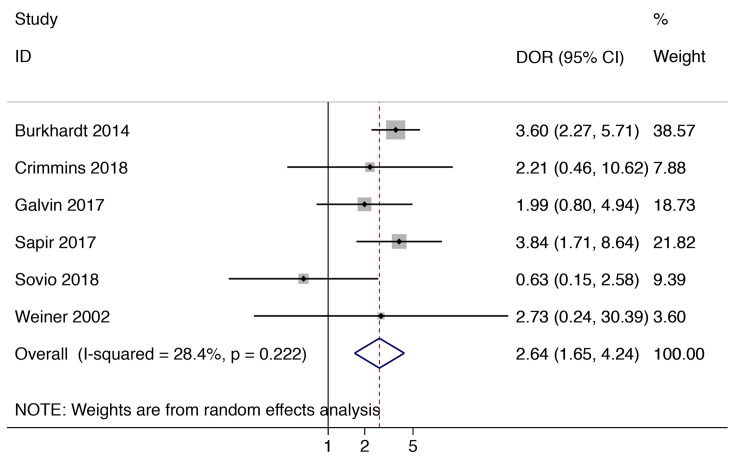
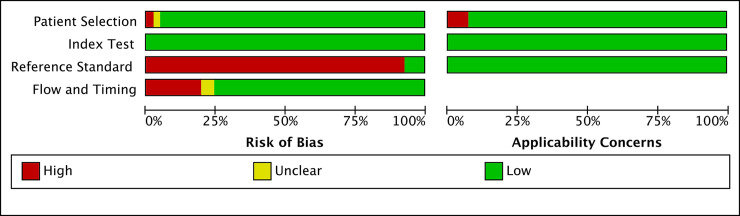
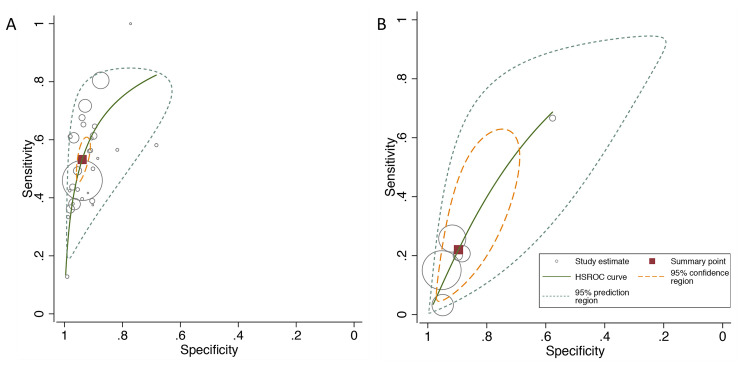
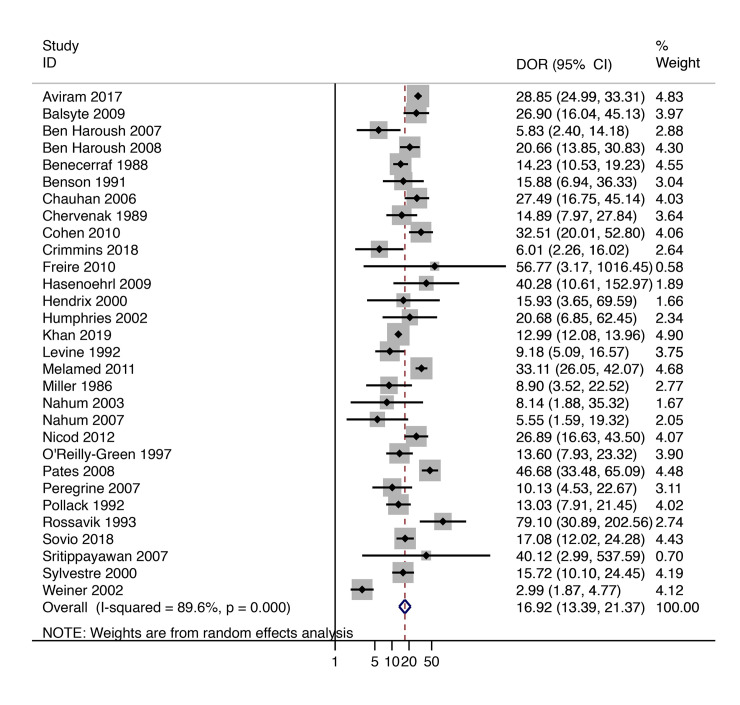
We conducted a predefined literature search in Medline, Excerpta Medica database (EMBASE), the Cochrane library and ClinicalTrials.gov from inception to May 2020. No language restrictions were applied. We included studies where the ultrasound was performed as part of universal screening and those that included low- and mixed-risk pregnancies and excluded studies confined to high risk pregnancies. We used the estimated fetal weight (EFW) (multiple formulas and thresholds) and the abdominal circumference (AC) to define suspected large for gestational age (LGA). Adverse perinatal outcomes included macrosomia (multiple thresholds), shoulder dystocia, and other markers of neonatal morbidity. The risk of bias was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool. Meta-analysis was carried out using the hierarchical summary receiver operating characteristic (ROC) and the bivariate logit-normal (Reitsma) models. We identified 41 studies that met our inclusion criteria involving 112,034 patients in total. These included 11 prospective cohort studies (N = 9986), one randomized controlled trial (RCT) (N = 367), and 29 retrospective cohort studies (N = 101,681). The quality of the studies was variable, and only three studies blinded the ultrasound findings to the clinicians. Both EFW >4,000 g (or 90th centile for the gestational age) and AC >36 cm (or 90th centile) had >50% sensitivity for predicting macrosomia (birthweight above 4,000 g or 90th centile) at birth with positive likelihood ratios (LRs) of 8.74 (95% confidence interval [CI] 6.84-11.17) and 7.56 (95% CI 5.85-9.77), respectively. There was significant heterogeneity at predicting macrosomia, which could reflect the different study designs, the characteristics of the included populations, and differences in the formulas used. An EFW >4,000 g (or 90th centile) had 22% sensitivity at predicting shoulder dystocia with a positive likelihood ratio of 2.12 (95% CI 1.34-3.35). There was insufficient data to analyze other markers of neonatal morbidity.
In this study, we found that suspected LGA is strongly predictive of the risk of delivering a large infant in low- and mixed-risk populations. However, it is only weakly (albeit statistically significantly) predictive of the risk of shoulder dystocia. There was insufficient data to analyze other markers of neonatal morbidity.
巨大儿筛查的效果尚未得到充分证实。一个有效的筛查项目的关键要素之一是测试预测该疾病的准确性。本研究旨在调查在低风险和混合风险人群中,超声胎儿生物测量在预测巨大儿分娩、肩难产和相关新生儿发病率方面的诊断效果。
我们在 Medline、Excerpta Medica 数据库(EMBASE)、Cochrane 图书馆和 ClinicalTrials.gov 中进行了预先设定的文献检索,检索时间从开始到 2020 年 5 月。未应用语言限制。我们纳入了作为常规筛查一部分进行的超声检查研究,以及纳入了低风险和混合风险妊娠的研究,并排除了仅针对高风险妊娠的研究。我们使用估计胎儿体重(EFW)(多种公式和阈值)和腹围(AC)来定义疑似大于胎龄(LGA)。围产期不良结局包括巨大儿(多个阈值)、肩难产和其他新生儿发病率的标志物。使用诊断准确性研究的质量评估(QUADAS-2)工具评估偏倚风险。使用分层汇总受试者工作特征(ROC)和双变量对数正态(Reitsma)模型进行荟萃分析。我们确定了 41 项符合纳入标准的研究,共涉及 112,034 名患者。这些研究包括 11 项前瞻性队列研究(N=9986)、一项随机对照试验(RCT)(N=367)和 29 项回顾性队列研究(N=101,681)。研究质量参差不齐,只有三项研究将超声结果对临床医生进行了盲法。EFW>4000g(或胎龄 90 百分位)和 AC>36cm(或 90 百分位)对预测出生时大于 4000g 或 90 百分位的巨大儿(出生体重)的敏感性均超过 50%,阳性似然比(LR)分别为 8.74(95%置信区间 [CI] 6.84-11.17)和 7.56(95% CI 5.85-9.77)。在预测巨大儿方面存在显著异质性,这可能反映了不同的研究设计、纳入人群的特征以及使用的公式的差异。EFW>4000g(或 90 百分位)预测肩难产的敏感性为 22%,阳性似然比为 2.12(95% CI 1.34-3.35)。没有足够的数据来分析其他新生儿发病率的标志物。
在这项研究中,我们发现疑似 LGA 强烈预测了低风险和混合风险人群中分娩巨大儿的风险。然而,它对肩难产风险的预测仅(尽管具有统计学意义)微弱。没有足够的数据来分析其他新生儿发病率的标志物。