Department of Intensive Care, Sklifosovsky Research Institute of Emergency Medicine of the Moscow Healthcare Department, Moscow, Russia.
Department of Intensive Care, State Research Center-Burnasyan Federal Medical Biophysical Center of Federal Medical Biological Agency, Moscow, Russia.
PLoS One. 2020 Oct 13;15(10):e0240117. doi: 10.1371/journal.pone.0240117. eCollection 2020.
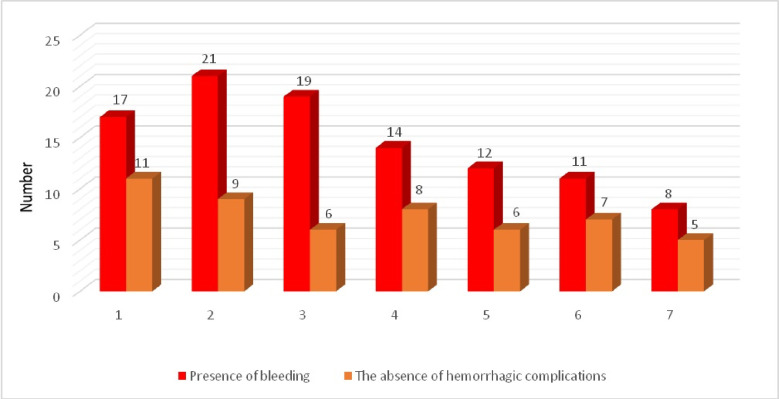
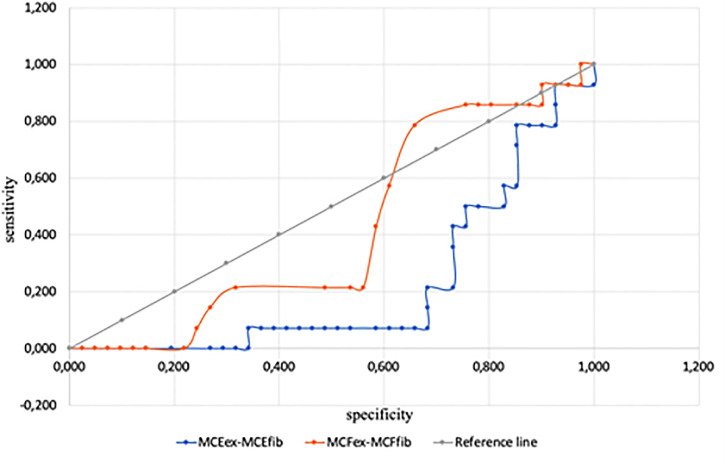
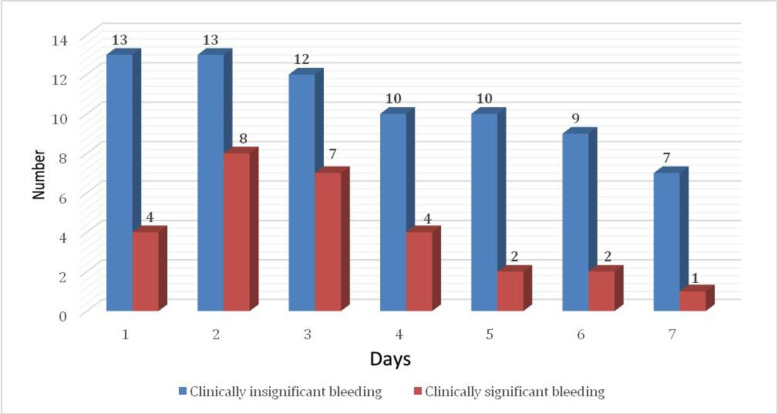
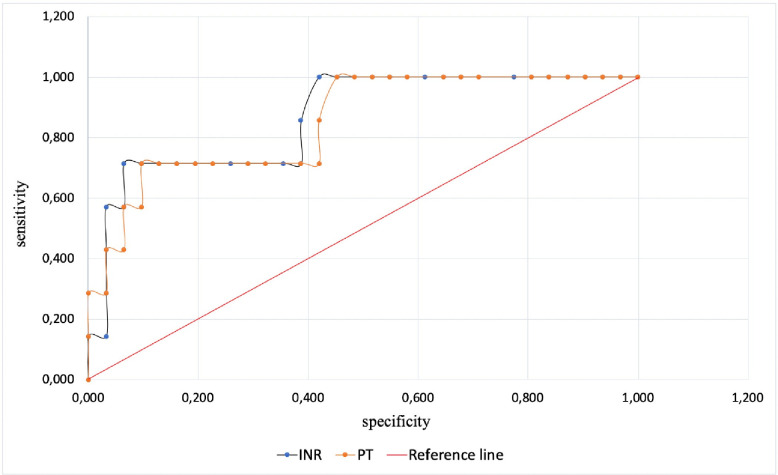
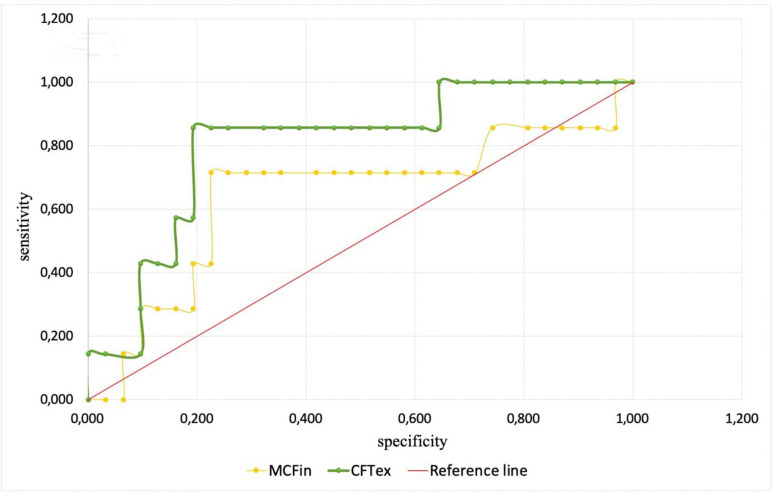
Extracorporeal membrane oxygenation (ECMO) is increasingly used to treat severe cases of acute respiratory or cardiac failure. Hemorrhagic complications represent one of the most common complications during ECMO, and can be life threatening. The purpose of this study was to elucidate pathophysiological mechanisms of ECMO-associated hemorrhagic complications and their impact on standard and viscoelastic coagulation tests. The study cohort included 27 patients treated with VV-ECMO or VA-ECMO. Hemostasis was evaluated using standard coagulation tests and viscoelastic parameters investigated with rotational thromboelastometry. Anticoagulation and hemorrhagic complications were analyzed for up to seven days depending on ECMO duration. Hemorrhagic complications developed in 16 (59%) patients. There were 102 discrete hemorrhagic episodes among 116 24-hour-intervals, of which 27% were considered to be clinically significant. The highest number of ECMO-associated hemorrhages occurred on the 2nd and 3rd day of treatment. Respiratory tract bleeding was the most common hemorrhagic complication, occurring in 62% of the 24-hour intervals. All 24-hours-intervals were divided into two groups: "with bleeding" and "without bleeding". The probability of hemorrhage was significantly associated with abnormalities of four parameters: increased international normalized ratio (INR, sensitivity 71%, specificity 94%), increased prothrombin time (PT, sensitivity 90%, specificity 72%), decreased intrinsic pathway maximal clot firmness (MCFin, sensitivity 76%, specificity 89%), and increased extrinsic pathway clot formation time (CFTex, sensitivity 77%, specificity 87%). In conclusions, early ECMO-associated hemorrhagic complications are related to one traditional and two novel viscoelastic coagulation abnormalities: PT/INR elevation, reduced maximum clot firmness due to intrinsic pathway dysfunction (MCFin), and prolonged clot formation time due to extrinsic pathway dysfunction (CFTex). When managing hemostasis during ECMO, derangements in PT/INR, MCFin and CFTex should be focused on.
体外膜肺氧合(ECMO)越来越多地用于治疗严重的急性呼吸或心脏衰竭。出血并发症是 ECMO 过程中最常见的并发症之一,可能危及生命。本研究的目的是阐明 ECMO 相关出血并发症的病理生理机制及其对标准和黏弹性凝血测试的影响。研究队列包括 27 名接受 VV-ECMO 或 VA-ECMO 治疗的患者。使用标准凝血测试评估止血情况,并使用旋转血栓弹性测定法研究黏弹性参数。根据 ECMO 持续时间,分析抗凝和出血并发症,最长可达 7 天。16 名(59%)患者发生出血并发症。在 116 个 24 小时间隔中有 102 个离散出血事件,其中 27%被认为具有临床意义。治疗第 2 天和第 3 天 ECMO 相关出血的发生率最高。呼吸道出血是最常见的出血并发症,占 24 小时间隔的 62%。所有 24 小时间隔均分为两组:“有出血”和“无出血”。出血的可能性与四个参数的异常显著相关:国际标准化比值(INR)升高(敏感性 71%,特异性 94%)、凝血酶原时间(PT)延长(敏感性 90%,特异性 72%)、内源性途径最大血凝块硬度降低(MCFin,敏感性 76%,特异性 89%)和外源性途径凝血形成时间(CFTex)延长(敏感性 77%,特异性 87%)。总之,早期 ECMO 相关出血并发症与一个传统和两个新的黏弹性凝血异常相关:PT/INR 升高、内源性途径功能障碍导致最大血凝块硬度降低(MCFin)以及外源性途径功能障碍导致凝血形成时间延长(CFTex)。在 ECMO 期间进行止血管理时,应重点关注 PT/INR、MCFin 和 CFTex 的异常。