Peng Yuting, Lin Peng, Wu Linyong, Wan Da, Zhao Yujia, Liang Li, Ma Xiaoyu, Qin Hui, Liu Yichen, Li Xin, Wang Xinrong, He Yun, Yang Hong
Department of Medical Ultrasonics, The First Affiliated Hospital of Guangxi Medical University, Nanning, China.
GE Healthcare, Shanghai, China.
Front Oncol. 2020 Sep 24;10:1646. doi: 10.3389/fonc.2020.01646. eCollection 2020.
Preoperative identification of hepatocellular carcinoma (HCC), combined hepatocellular-cholangiocarcinoma (cHCC-ICC), and intrahepatic cholangiocarcinoma (ICC) is essential for treatment decision making. We aimed to use ultrasound-based radiomics analysis to non-invasively distinguish histopathological subtypes of primary liver cancer (PLC) before surgery.
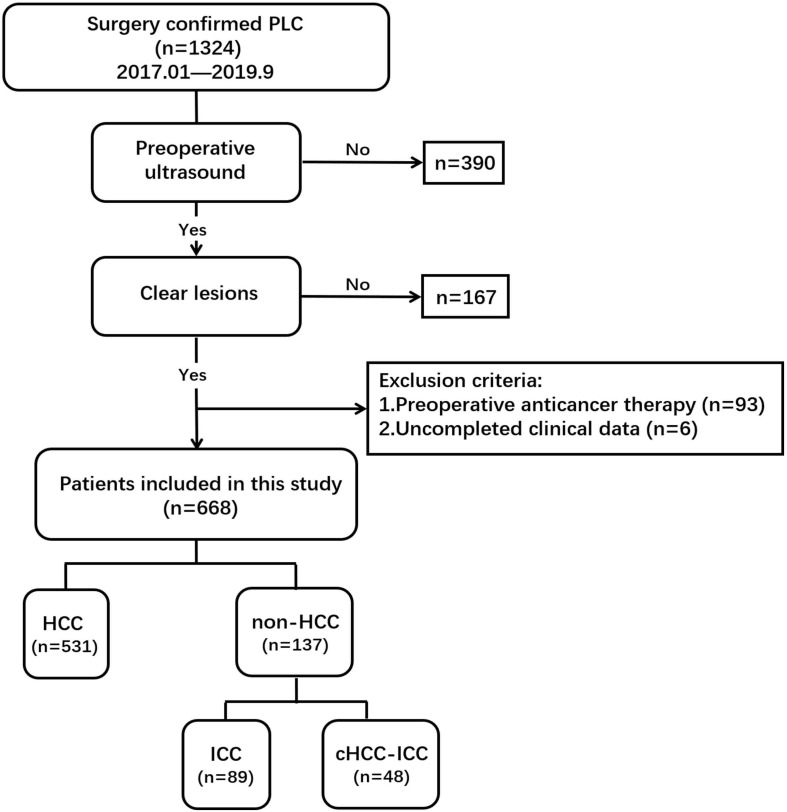
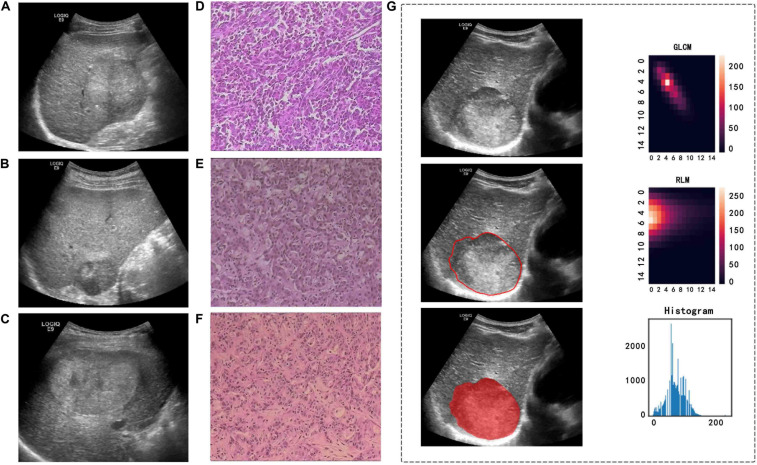
We retrospectively analyzed ultrasound images of 668 PLC patients, comprising 531 HCC patients, 48 cHCC-ICC patients, and 89 ICC patients. The boundary of a tumor was manually determined on the largest imaging slice of the ultrasound medicine image by ITK-SNAP software (version 3.8.0), and then, the high-throughput radiomics features were extracted from the obtained region of interest (ROI) of the tumor. The combination of different dimension-reduction technologies and machine learning approaches was used to identify important features and develop the moderate radiomics model. The comprehensive ability of the radiomics model can be evaluated by the area under the receiver operating characteristic curve (AUC).
After digitally processing tumor ultrasound images, 5,234 high-throughput radiomics features were obtained. We used the Spearman + least absolute shrinkage and selection operator (LASSO) regression method for feature selection and logistics regression for modeling to develop the HCC-vs-non-HCC radiomics model (composed of 16 features). The Spearman + statistical test + random forest methods were used for feature selection, and logistics regression was applied for modeling to develop the ICC-vs-cHCC-ICC radiomics model (composed of 19 features). The overall performance of the radiomics model in identifying different histopathological types of PLC was moderate, with AUC values of 0.854 (training cohort) and 0.775 (test cohort) in the HCC-vs-non-HCC radiomics model and 0.920 (training cohort) and 0.728 (test cohort) in the ICC-vs-cHCC-ICC radiomics model.
Ultrasound-based radiomics models can help distinguish histopathological subtypes of PLC and provide effective clinical decision making for the accurate diagnosis and treatment of PLC.
术前鉴别肝细胞癌(HCC)、肝内胆管癌(ICC)和肝细胞胆管癌(cHCC-ICC)对于治疗决策至关重要。我们旨在利用基于超声的放射组学分析在术前非侵入性地区分原发性肝癌(PLC)的组织病理学亚型。
我们回顾性分析了668例PLC患者的超声图像,其中包括531例HCC患者、48例cHCC-ICC患者和89例ICC患者。通过ITK-SNAP软件(版本3.8.0)在超声医学图像的最大成像切片上手动确定肿瘤边界,然后从获得的肿瘤感兴趣区域(ROI)中提取高通量放射组学特征。采用不同降维技术和机器学习方法的组合来识别重要特征并建立中度放射组学模型。放射组学模型的综合能力可通过受试者操作特征曲线(AUC)下的面积来评估。
对肿瘤超声图像进行数字处理后,获得了5234个高通量放射组学特征。我们使用Spearman+最小绝对收缩和选择算子(LASSO)回归方法进行特征选择,并使用逻辑回归进行建模,以建立HCC与非HCC放射组学模型(由16个特征组成)。使用Spearman+统计检验+随机森林方法进行特征选择,并应用逻辑回归进行建模,以建立ICC与cHCC-ICC放射组学模型(由19个特征组成)。放射组学模型在识别PLC不同组织病理学类型方面的总体表现中等,在HCC与非HCC放射组学模型中,训练队列的AUC值为0.854,测试队列的AUC值为0.775;在ICC与cHCC-ICC放射组学模型中,训练队列的AUC值为0.920,测试队列的AUC值为0.728。
基于超声的放射组学模型有助于区分PLC的组织病理学亚型,并为PLC的准确诊断和治疗提供有效的临床决策。