Department of Nuclear Medicine, University Hospital Zurich, University of Zurich, Rämistrasse 100, 8091, Zürich, Switzerland.
Department of Urology, University Hospital Zurich, University of Zurich, Zurich, Switzerland.
Eur J Nucl Med Mol Imaging. 2021 Apr;48(4):1219-1228. doi: 10.1007/s00259-020-05058-5. Epub 2020 Oct 19.
Positron emission tomography (PET) targeting the prostate-specific membrane antigen (PSMA) has superior sensitivity over conventional imaging (CI) to stage prostate cancer (PCa) and therefore is increasingly used in staging to stratify patients before radical therapy. Whether this improved diagnostic accuracy translates into improved outcome after radical prostatectomy (RPE) has not yet been shown. Therefore, the aim of this study was to compare the oncological outcome after RPE between patients that underwent preoperative staging with CI or PSMA-PET for intermediate and high-risk PCa.
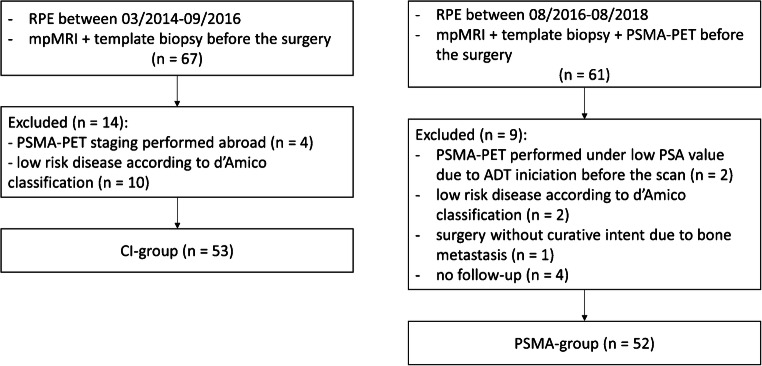
We retrospectively selected all patients that underwent RPE for intermediate- or high-risk PCa at our institution before PSMA-PET introduction (between March 2014 and September 2016) and compared the oncologic outcome of patients staged with PSMA-PET (between October 2016 and October 2018). Oncological pre-surgical risk parameters (age, PSA, D'Amico score, biopsy-ISUP, and cT stage) were compared between the groups. Oncological outcome was determined as PSA persistence, nerve-sparing rate, and surgical margin status. Wilcoxon rank-sum, Fisher's, and chi-square tests where used for statistical testing.
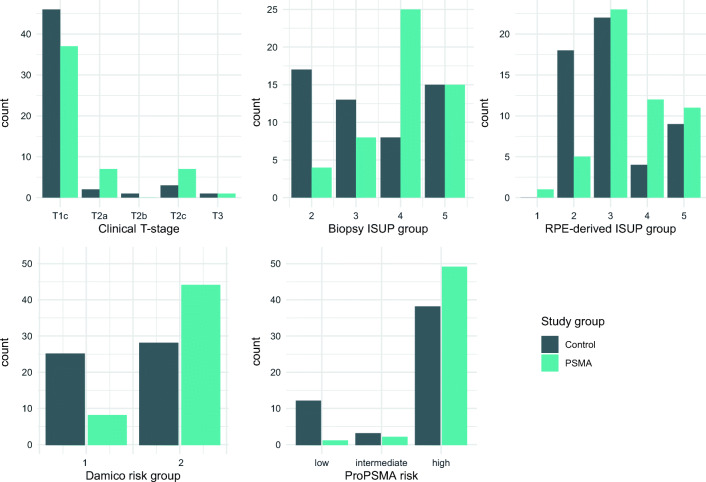
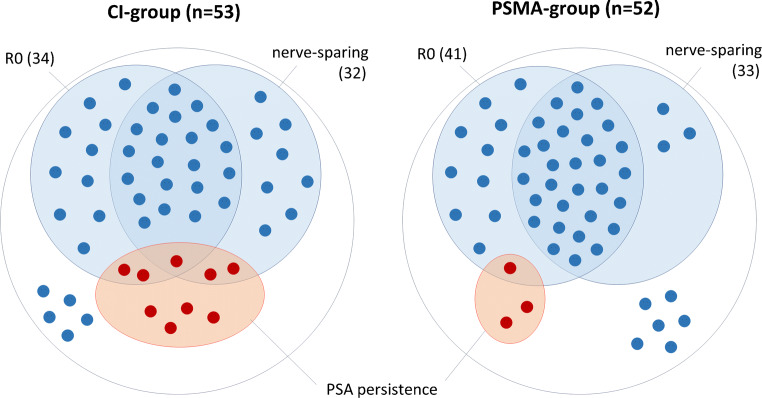
One hundred five patients were included, 53 in the CI group and 52 in the PSMA-group. Patients in the PSMA group had higher ISUP grade (p < 0.001) and D'Amico score (p < 0.05). The rate of free surgical margins and PSA persistence after RPE was 64% and 17% for the CI and 77% and 6% for the PSMA group (p = 0.15 and 0.13, respectively). Subgroup analysis with high-risk patients revealed PSA persistence in 7% (3/44) in the PSMA group and 25% (7/28) in the CI group (p = 0.04). Limitations include the retrospective design and choline-PET for some patients in the CI group.
Immediate outcome after RPE was not worse in the PSMA group compared with the CI group, despite a higher-risk cohort. In a comparison of only high-risk patients, PSMA-PET staging was associated with a significantly lower rate of postsurgical PSA persistence.
与传统影像学(CI)相比,正电子发射断层扫描(PET)靶向前列腺特异性膜抗原(PSMA)在诊断前列腺癌(PCa)方面具有更高的敏感性,因此越来越多地用于分期,以便在根治性治疗前对患者进行分层。然而,PSMA-PET 术前分期是否能提高根治性前列腺切除术(RPE)后的生存结果,目前尚未得到证实。因此,本研究旨在比较接受中高危 PCa 治疗的患者在接受 CI 或 PSMA-PET 术前分期后,RPE 后的肿瘤学结果。
我们回顾性地选择了在 PSMA-PET 引入之前(2014 年 3 月至 2016 年 9 月)在我们机构接受中高危 PCa 治疗的所有 RPE 患者,并比较了接受 PSMA-PET 分期的患者(2016 年 10 月至 2018 年 10 月)的肿瘤学结果。比较了两组患者的术前肿瘤学风险参数(年龄、PSA、D'Amico 评分、活检-ISUP 和 cT 分期)。PSA 持续存在、神经保留率和手术切缘状态被确定为肿瘤学预后参数。Wilcoxon 秩和检验、Fisher 确切概率检验和卡方检验用于统计学检验。
共纳入 105 例患者,其中 CI 组 53 例,PSMA 组 52 例。PSMA 组的 ISUP 分级(p<0.001)和 D'Amico 评分(p<0.05)更高。RPE 后无肿瘤切缘和 PSA 持续存在的比例分别为 CI 组 64%和 17%,PSMA 组 77%和 6%(p=0.15 和 0.13)。高危患者亚组分析显示,PSMA 组 PSA 持续存在率为 7%(3/44),CI 组为 25%(7/28)(p=0.04)。局限性包括回顾性设计和 CI 组中一些患者使用胆碱 PET。
尽管高危患者比例较高,但与 CI 组相比,PSMA 组的 RPE 后即刻结果并不差。在仅比较高危患者的情况下,PSMA-PET 分期与术后 PSA 持续存在的发生率显著降低相关。