Baral Suman, Chhetri Raj Kumar, Gyawali Milan, Thapa Neeraj
Department of Surgery, Lumbini Medical College and Teaching Hospital Ltd, Tansen-7, Pravas, Palpa, Nepal.
Int J Surg Case Rep. 2020;75:492-496. doi: 10.1016/j.ijscr.2020.09.145. Epub 2020 Sep 24.
Splenic abscess generally occurs through hematogenous spread and typically follows endocarditis or seeding from contiguous sites of infection. This can be complicated by empyema thoracis. We present a rarer case of chronic alcoholic with splenic abscess along with empyema thoracis.
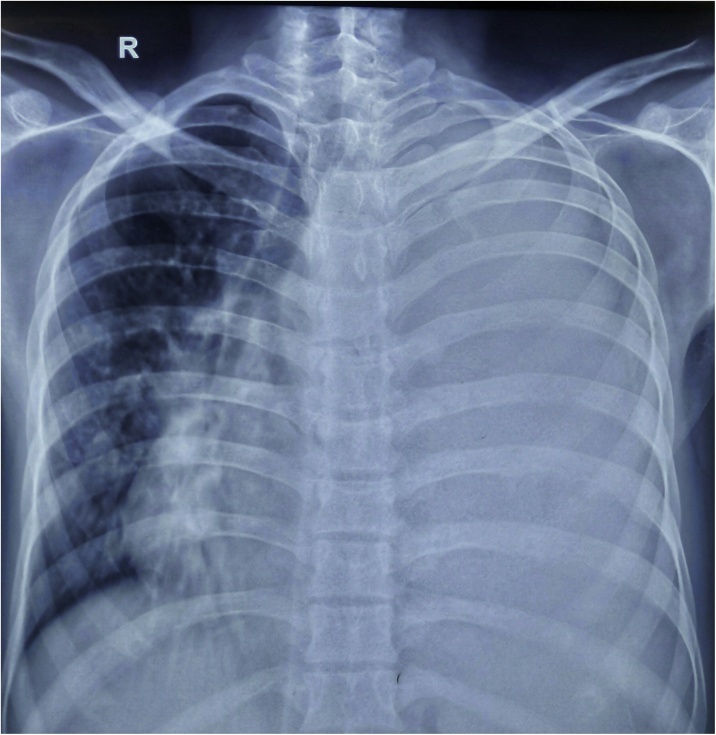
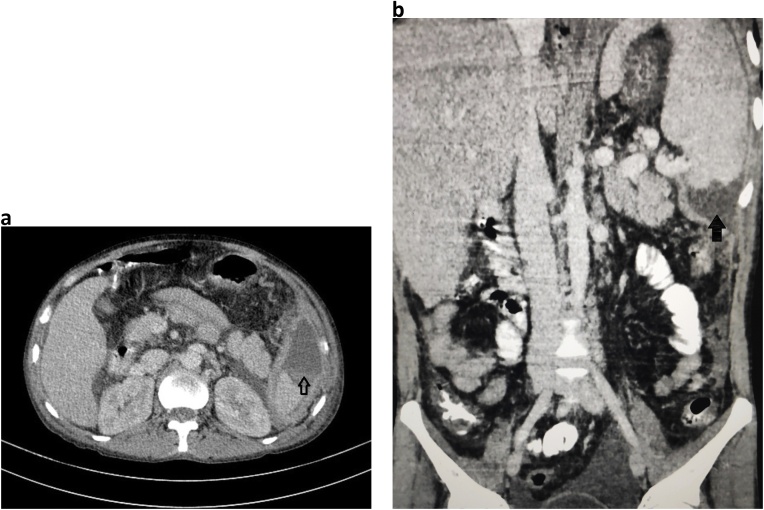
A 39-year old alcoholic male presented with history of pain at left hypochondrium and difficulty breathing for 7 days. Abdominal examination revealed tenderness at left hypochondrium along with enlarged spleen and liver associated with decreased air entry of left chest. Chest X-ray showed complete white out lung field on left side. Contrast enhanced tomography abdomen and pelvis revealed splenic abscess involving lower pole of spleen along with peri splenic extension. Tube thoracostomy drainage on left chest was done followed by ultrasonography guided repeated aspiration of splenic entity. Pus culture sensitivity showed growth of Streptococcus pyogenes while splenic aspirate remained sterile. Patient got discharged on 8th day of admission with full recovery.
Splenic abscess is the rare entity which is commonly seen in immunocompromised individuals that might get complicated as empyema thoracis and management includes broad spectrum antibiotics along with tube thoracostomy and percutaneous drainage of splenic abscess if possible, in view of spleen being salvageable. Pleural collection revealed growth of Streptococcus pyogenes in our case which itself is the rare finding.
Splenic abscess can be managed with percutaneous aspiration/drainage if lesion is unilocular in the view of salvaging spleen. Complicated empyema can be managed with tube thoracostomy along with broad spectrum antibiotics.
脾脓肿通常通过血行播散发生,典型情况是继发于心内膜炎或邻近感染部位的菌血症。这可能并发脓胸。我们报告一例较为罕见的病例,一名慢性酒精中毒患者同时患有脾脓肿和脓胸。
一名39岁男性酒精中毒患者,有左季肋部疼痛和呼吸困难7天的病史。腹部检查发现左季肋部压痛,脾脏和肝脏肿大,同时左胸呼吸音减弱。胸部X线显示左侧肺野完全变白。腹部和盆腔增强CT显示脾脓肿累及脾下极并伴有脾周扩展。对左侧胸部进行了胸腔闭式引流,随后在超声引导下对脾脏肿物进行反复穿刺抽吸。脓液培养药敏显示化脓性链球菌生长,而脾脏穿刺液无菌。患者入院第8天出院,已完全康复。
脾脓肿是一种罕见疾病,常见于免疫功能低下的个体,可能并发脓胸,治疗包括使用广谱抗生素,以及在脾脏可挽救的情况下进行胸腔闭式引流和经皮脾脓肿引流。在我们的病例中,胸腔积液培养出化脓性链球菌,这本身就是一个罕见的发现。
如果脾脓肿为单房性,为挽救脾脏,可采用经皮穿刺抽吸/引流进行治疗。复杂的脓胸可通过胸腔闭式引流和广谱抗生素进行治疗。