Yao Jie, Chang Zhibo, Zhu Lin, Fan Junqiang
Department of Thoracic Surgery, Second Affiliated Hospital of Zhejiang University, School of Medicine, Hangzhou, China.
Medicine (Baltimore). 2020 Oct 16;99(42):e22719. doi: 10.1097/MD.0000000000022719.
To compare perioperative outcomes and surgeon physical and mental stress when performing lobectomy through uniportal and multiportal video-assisted thoracoscopic surgery (VATS) on patients with non-small-cell lung cancer (NSCLC).
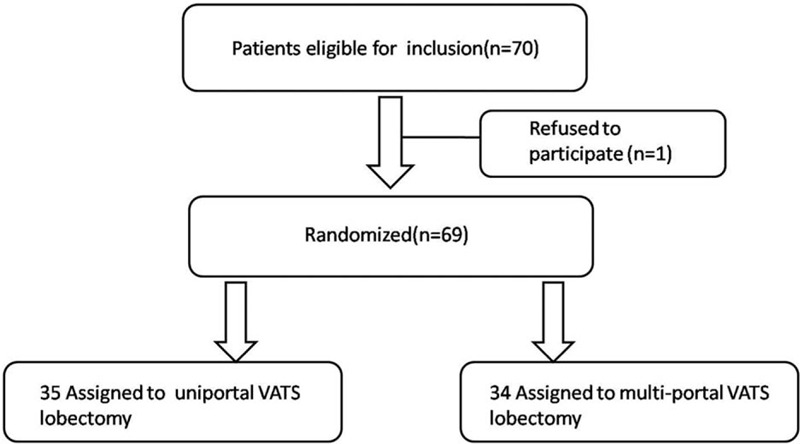
Patients aged 41 to 73 years with resectable NSCLC were randomly assigned via a computer-generated randomisation sequence to receive either uniportal VATS (UVATS) or multiportal VATS (MVATS) lobectomy and lymphadenectomy between December 2015 and October 2016. Overall, we randomly assigned 35 patients to the UVATS and 34 to the MVATS group. Patients and the investigators undertaking interventions, assessing short-term outcomes, performing ergonomic evaluations, and analyzing data were not masked to group assignment.
Patient demographics of the 2 groups were comparable. The ergonomic evaluation considered eye blink rate and the NASA Task Load Index (NASA-TLX), better results were observed in UVATS than in MVATS. The operative time, number of lymph nodes harvested, chest tube duration, length of hospital stay, and lung function were not significantly different between the groups. Compared with MVATS lobectomy, UVATS lobectomy was associated with less intraoperative blood loss and less volume of total drainage in the 24 hours. No conversion, no reoperation, and no in-hospital mortality occurred in either group.
UVATS lobectomy is a safe and programmable technique with some better perioperative outcomes and ergonomic results than MVATS. Further studies based on large numbers of patients and with long-term follow-up are required to confirm its benefits towards patients.
ClinicalTrials.gov ID:NCT02462356. Registered May 27, 2015.
比较非小细胞肺癌(NSCLC)患者接受单孔与多孔电视辅助胸腔镜手术(VATS)肺叶切除术时的围手术期结局以及外科医生的身心压力。
2015年12月至2016年10月期间,将年龄在41至73岁之间、可切除的NSCLC患者通过计算机生成的随机序列随机分配,分别接受单孔VATS(UVATS)或多孔VATS(MVATS)肺叶切除术及淋巴结清扫术。总体而言,我们将35例患者随机分配至UVATS组,34例患者随机分配至MVATS组。进行干预、评估短期结局、进行人体工程学评估及分析数据的患者和研究人员未对分组情况进行设盲。
两组患者的人口统计学特征具有可比性。人体工程学评估考虑了眨眼率和美国国家航空航天局任务负荷指数(NASA-TLX),结果显示UVATS组优于MVATS组。两组间手术时间、清扫淋巴结数量、胸管留置时间、住院时间及肺功能无显著差异。与MVATS肺叶切除术相比,UVATS肺叶切除术术中失血量更少,术后24小时总引流量更少。两组均未发生中转、再次手术及院内死亡。
UVATS肺叶切除术是一种安全且可规划的技术,其围手术期结局和人体工程学结果优于MVATS。需要基于大量患者并进行长期随访的进一步研究来证实其对患者的益处。
ClinicalTrials.gov标识符:NCT02462356。于2015年5月27日注册。