Gibson Alice A, Eroglu Elif I, Rooney Kieron, Harper Claudia, McClintock Sally, Franklin Janet, Markovic Tania P, Seimon Radhika V, Sainsbury Amanda
Boden Collaboration for Obesity, Nutrition, Exercise and Eating Disorders, Faculty of Medicine and Health The University of Sydney Camperdown New South Wales Australia.
The Menzies Centre for Health Policy, School of Public Health, Faculty of Medicine and Health The University of Sydney Camperdown New South Wales Australia.
Obes Sci Pract. 2020 Jun 10;6(5):544-551. doi: 10.1002/osp4.432. eCollection 2020 Oct.
Detection of the mild ketosis induced by severely energy-restricted diets may be a clinically useful way to monitor and promote dietary adherence. Mild ketosis is often assessed using urine dipsticks, but accuracy for this purpose has not been tested.
To determine the accuracy of urine dipsticks to detect mild ketosis during adherence to a severely energy-restricted diet.
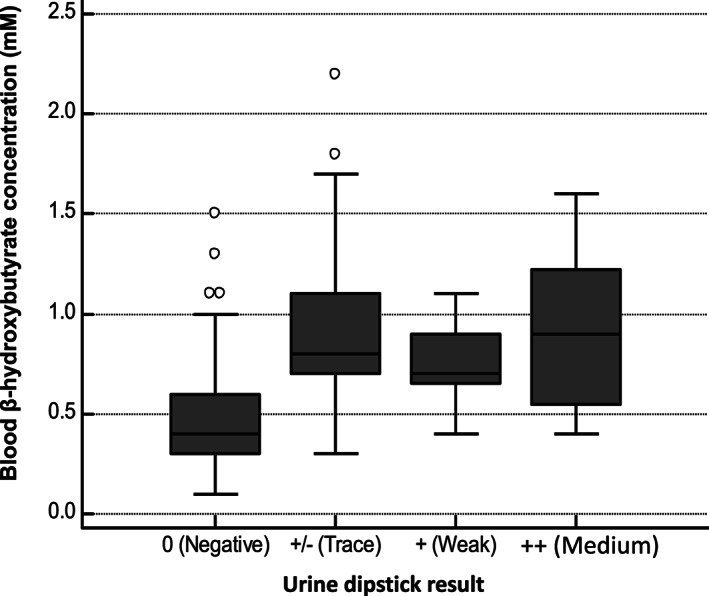
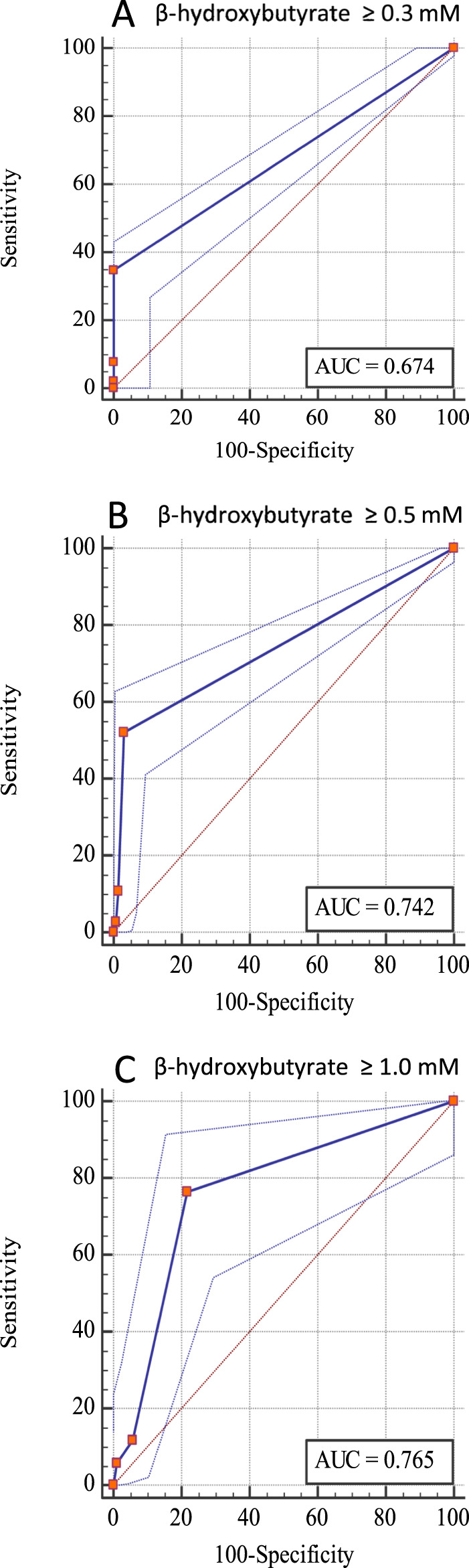
Two hundred and sixty three (263) fasting urine and 263 fasting blood samples were taken from 50 women (mean [standard deviation, SD] age 58.0 [4.3] years and body mass index 34.3 [2.4] kg/m) before and at six time points during or for up to 10 weeks after 16 weeks of severe energy restriction, achieved with a total meal replacement diet. The amount of ketones (acetoacetate) in the urine was classified as '0 (Negative)', '+/- (Trace)', '+ (Weak)' or '++ (Medium)' by urine dipsticks (Ketostix, Bayer). The concentration of ketones (β-hydroxybutyrate) in the blood was measured with our reference method, a portable ketone monitor (FreeStyle Optium, Abbott). The diagnostic accuracy of the urine dipsticks was assessed from the percent of instances when a person was actually 'in ketosis' (as defined by a blood β-hydroxybutyrate concentration at or above three different thresholds) that were also identified by the urine dipsticks as being from a person in ketosis (the percent 'true positives' or sensitivity), as well as the percent of instances when a person was not in ketosis (as defined by the blood monitor result) was correctly identified as such with the urine dipstick (the percent 'true negatives' or specificity). Thresholds of ≥0.3mM, ≥0.5mM or ≥1.0mM were selected, because mean blood concentrations of β-hydroxybutyrate during ketogenic diets are approximately 0.5mM. Sensitivity and specificity were then used to generate receiver operating characteristic curves, with the area under these curves indicating the ability of the dipsticks to correctly identify people in ketosis (1 = perfect results, 0.5 = random results).
At threshold blood β-hydroxybutyrate concentrations of ≥0.3mM, ≥0.5mM and ≥1.0mM, the sensitivity of the urine dipsticks was 35%, 52% and 76%; the specificity was 100%, 97% and 78%; and the area under the receiver operating characteristic curves was 0.67, 0.74 and 0.77, respectively. These low levels of sensitivity mean that 65%, 48% or 24% of the instances when a person was in ketosis were not detected by the urine dipsticks.
Urine dipsticks are not an accurate or clinically useful means of detecting mild ketosis in people undergoing a severely energy-restricted diet and should thus not be recommended in clinical treatment protocols. If monitoring of mild ketosis is indicated (eg, to monitor or help promote adherence to a severely energy-restricted diet), then blood monitors should be used instead.
检测由严格能量限制饮食引起的轻度酮症可能是一种临床上用于监测和促进饮食依从性的有用方法。轻度酮症通常使用尿试纸进行评估,但尚未对其用于此目的的准确性进行测试。
确定在严格能量限制饮食期间,尿试纸检测轻度酮症的准确性。
从50名女性(平均[标准差,SD]年龄58.0[4.3]岁,体重指数34.3[2.4]kg/m²)中采集了263份空腹尿液和263份空腹血液样本,在采用全代餐饮食实现16周严格能量限制之前以及之后的6个时间点(持续或长达10周)进行采集。尿试纸(酮体试纸,拜耳公司)将尿液中的酮体(乙酰乙酸)量分为“0(阴性)”、“+/-(微量)”、“+(弱阳性)”或“++(中等阳性)”。采用我们的参考方法,即便携式酮体监测仪(自由风格血糖仪,雅培公司)测量血液中的酮体(β-羟基丁酸)浓度。根据尿试纸将实际“处于酮症状态”(由血液β-羟基丁酸浓度达到或高于三个不同阈值定义)的人识别为处于酮症状态的实例百分比(“真阳性”百分比或灵敏度),以及尿试纸将未处于酮症状态(由血液监测结果定义)正确识别为未处于酮症状态的实例百分比(“真阴性”百分比或特异性),评估尿试纸的诊断准确性。选择≥0.3mM、≥0.5mM或≥1.0mM的阈值,因为生酮饮食期间β-羟基丁酸的平均血液浓度约为0.5mM。然后使用灵敏度和特异性生成受试者工作特征曲线,这些曲线下的面积表明尿试纸正确识别处于酮症状态的人的能力(1 = 完美结果,0.5 = 随机结果)。
在血液β-羟基丁酸浓度阈值≥0.3mM、≥0.5mM和≥1.0mM时,尿试纸的灵敏度分别为35%、52%和76%;特异性分别为100%、97%和78%;受试者工作特征曲线下的面积分别为0.67、0.74和0.77。这些低水平的灵敏度意味着尿试纸未检测到65%、48%或24%的处于酮症状态的实例。
尿试纸不是检测严格能量限制饮食人群中轻度酮症的准确或临床上有用的方法,因此不应在临床治疗方案中推荐。如果需要监测轻度酮症(例如,监测或帮助促进对严格能量限制饮食的依从性),则应改用血液监测仪。