Niederwanger Christian, Varga Thomas, Hell Tobias, Stuerzel Daniel, Prem Jennifer, Gassner Magdalena, Rickmann Franziska, Schoner Christina, Hainz Daniela, Cortina Gerard, Hetzer Benjamin, Treml Benedikt, Bachler Mirjam
Department of Pediatrics, Pediatrics I, Medical University of Innsbruck, Innsbruck, Austria.
Institute of Anaesthesiology, University of Zurich and University Hospital Zurich, Zurich, Switzerland.
PeerJ. 2020 Oct 5;8:e9993. doi: 10.7717/peerj.9993. eCollection 2020.
Scores can assess the severity and course of disease and predict outcome in an objective manner. This information is needed for proper risk assessment and stratification. Furthermore, scoring systems support optimal patient care, resource management and are gaining in importance in terms of artificial intelligence.
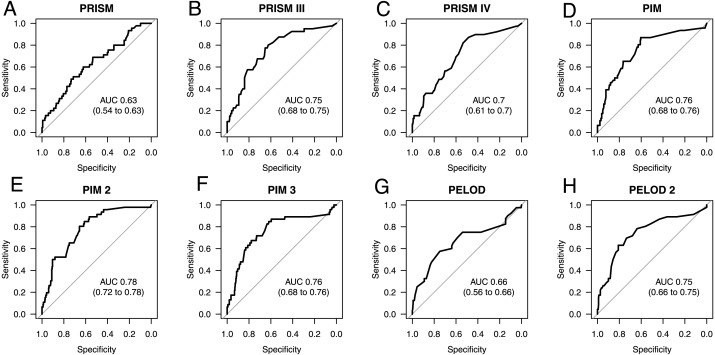
This study evaluated and compared the prognostic ability of various common pediatric scoring systems (PRISM, PRISM III, PRISM IV, PIM, PIM2, PIM3, PELOD, PELOD 2) in order to determine which is the most applicable score for pediatric sepsis patients in terms of timing of disease survey and insensitivity to missing data.
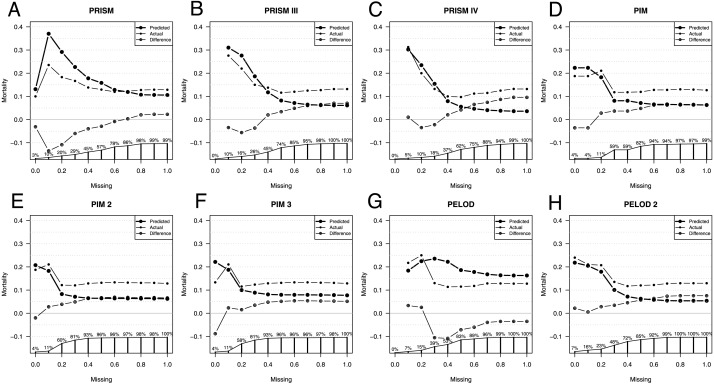
We retrospectively examined data from 398 patients under 18 years of age, who were diagnosed with sepsis. Scores were assessed at ICU admission and re-evaluated on the day of peak C-reactive protein. The scores were compared for their ability to predict mortality in this specific patient population and for their impairment due to missing data.
PIM (AUC 0.76 (0.68-0.76)), PIM2 (AUC 0.78 (0.72-0.78)) and PIM3 (AUC 0.76 (0.68-0.76)) scores together with PRSIM III (AUC 0.75 (0.68-0.75)) and PELOD 2 (AUC 0.75 (0.66-0.75)) are the most suitable scores for determining patient prognosis at ICU admission. Once sepsis is pronounced, PELOD 2 (AUC 0.84 (0.77-0.91)) and PRISM IV (AUC 0.8 (0.72-0.88)) become significantly better in their performance and count among the best prognostic scores for use at this time together with PRISM III (AUC 0.81 (0.73-0.89)). PELOD 2 is good for monitoring and, like the PIM scores, is also largely insensitive to missing values.
Overall, PIM scores show comparatively good performance, are stable as far as timing of the disease survey is concerned, and they are also relatively stable in terms of missing parameters. PELOD 2 is best suitable for monitoring clinical course.
评分能够客观评估疾病的严重程度和病程,并预测预后。这些信息对于进行恰当的风险评估和分层至关重要。此外,评分系统有助于实现最佳的患者护理和资源管理,并且在人工智能方面的重要性日益凸显。
本研究评估并比较了各种常见儿科评分系统(PRISM、PRISM III、PRISM IV、PIM、PIM2、PIM3、PELOD、PELOD 2)的预后能力,以确定就疾病调查时间和对缺失数据不敏感而言,哪种评分系统最适用于儿科脓毒症患者。
我们回顾性分析了398例18岁以下脓毒症确诊患者的数据。在重症监护病房(ICU)入院时评估评分,并在C反应蛋白峰值日重新评估。比较这些评分在预测该特定患者群体死亡率方面的能力以及因数据缺失导致的损害。
PIM(曲线下面积[AUC] 0.76[0.68 - 0.76])、PIM2(AUC 0.78[0.72 - 0.78])和PIM3(AUC 0.76[0.68 - 0.76])评分以及PRSIM III(AUC 0.75[0.68 - 0.75])和PELOD 2(AUC 0.75[0.66 - 0.75])是ICU入院时确定患者预后最合适的评分。一旦脓毒症确诊,PELOD 2(AUC 0.84[0.77 - 0.91])和PRISM IV(AUC 0.8[0.72 - 0.88])的表现显著更佳,与PRISM III(AUC 0.81[0.73 - 0.89])一同成为此时最佳的预后评分。PELOD 2适用于监测,并且与PIM评分一样,对缺失值也基本不敏感。
总体而言,PIM评分表现相对较好,在疾病调查时间方面较为稳定,在缺失参数方面也相对稳定。PELOD 2最适合监测临床病程。