Xie Hailun, Huang Shizhen, Yuan Guanghui, Kuang Jiaan, Yan Ling, Wei Lishuang, Tang Shuangyi, Gan Jialiang
Department of Colorectal and Anal Surgery, The First Affiliated Hospital, Guangxi Medical University, Nanning, Guangxi, P.R. China.
Department of Respiratory Medicine, The First Affiliated Hospital, Guangxi Medical University, Nanning, Guangxi, P.R. China.
PeerJ. 2020 Oct 8;8:e10100. doi: 10.7717/peerj.10100. eCollection 2020.
Several studies have proposed that the advanced lung cancer inflammation index (ALI), a new inflammation-related index, can be used for the prognosis assessment of various malignancies. However, few studies have reported its prognostic value in colorectal cancer (CRC). Therefore, this study explored the relationship between ALI and outcomes in CRC patients.
A total of 662 CRC patients who underwent surgery between 2012 and 2014 were included. The ALI was defined as: body mass index × serum albumin/neutrophil to lymphocyte ratio. The X-tile program identified the optimal cut-off value of ALI. Logistic regression analyses determined factors affecting postoperative complications. The Kaplan-Meier method and Cox proportional hazards analyses evaluated potential prognostic factors.
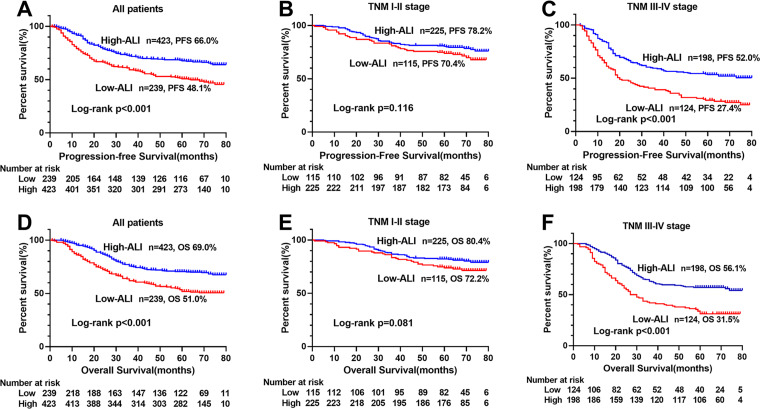
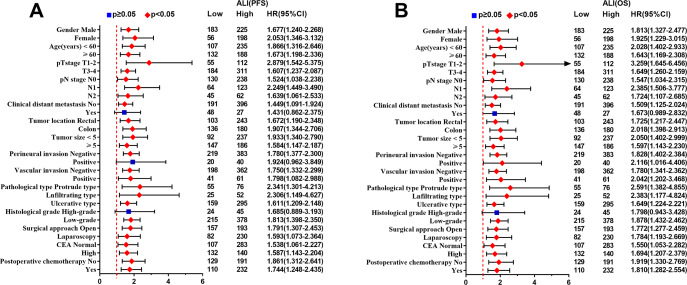
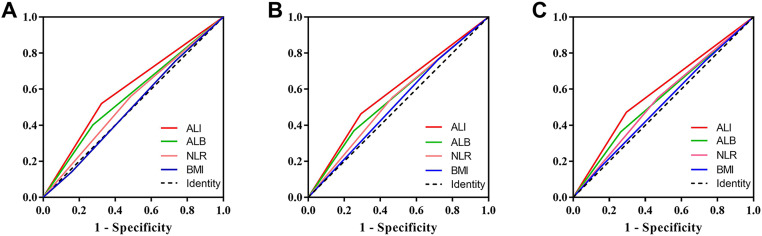
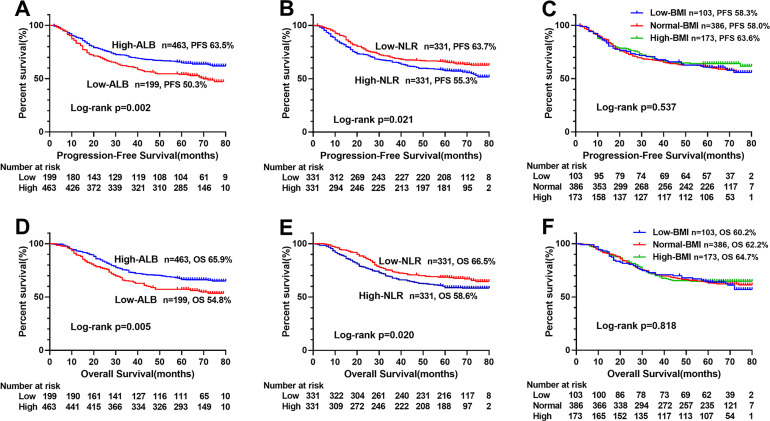
The optimal cut-off of ALI in males and females were 31.6 and 24.4, respectively. Low-ALI was an independent risk factor for postoperative complications in CRC patients (odds ratio: 1.933, 95% CI [1.283-2.911], = 0.002). Low-ALI groups also had significantly lower progression-free survival (PFS) and overall survival (OS), when compared with the high-ALI group, especially at advance tumor stages. Using multivariate analysis, ALI was determined as an independent prognostic factor for PFS (hazard ratio: 1.372, 95% CI [1.060-1.777], = 0.016) and OS (hazard ratio: 1.453, 95% confidence interval: 1.113-1.898, = 0.006).
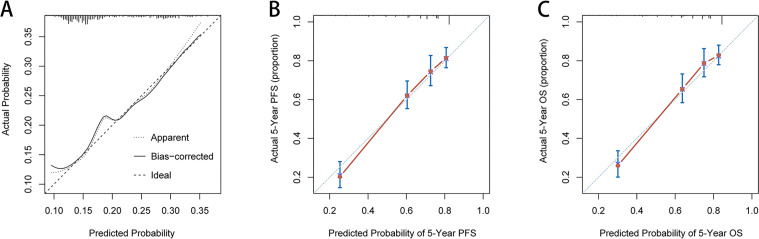
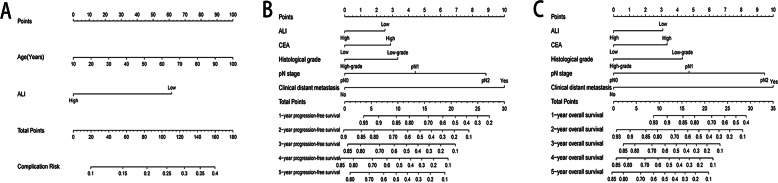
ALI is an independent predictor of short and long-term outcomes in CRC patients, especially at advance tumor stages. The ALI-based nomograms can provide accurate and individualized prediction of postoperative complication risk and survival for CRC patients.
多项研究表明,新型炎症相关指标——晚期肺癌炎症指数(ALI)可用于评估多种恶性肿瘤的预后。然而,鲜有研究报道其在结直肠癌(CRC)中的预后价值。因此,本研究探讨了ALI与CRC患者预后的关系。
纳入2012年至2014年间接受手术的662例CRC患者。ALI定义为:体重指数×血清白蛋白/中性粒细胞与淋巴细胞比值。X-tile程序确定ALI的最佳临界值。逻辑回归分析确定影响术后并发症的因素。Kaplan-Meier法和Cox比例风险分析评估潜在的预后因素。
男性和女性ALI的最佳临界值分别为31.6和24.4。低ALI是CRC患者术后并发症的独立危险因素(比值比:1.933,95%可信区间[1.283-2.911],P = 0.002)。与高ALI组相比,低ALI组的无进展生存期(PFS)和总生存期(OS)也显著降低,尤其是在肿瘤晚期。多因素分析显示,ALI是PFS(风险比:1.372,95%可信区间[1.060-1.777],P = 0.016)和OS(风险比:1.453,95%可信区间:1.113-1.898,P = 0.006)的独立预后因素。
ALI是CRC患者短期和长期预后的独立预测指标,尤其是在肿瘤晚期。基于ALI的列线图可为CRC患者术后并发症风险和生存提供准确的个体化预测。