Xie Hailun, Wei Lishuang, Liu Mingxiang, Liang Yanren, Yuan Guanghui, Gao Shunhui, Wang Qiwen, Lin Xin, Tang Shuangyi, Gan Jialiang
Department of Colorectal and Anal Surgery, The First Affiliated Hospital, Guangxi Medical University, Nanning, China.
Guangxi Key Laboratory of Enhanced Recovery After Surgery for Gastrointestinal Cancer, Nanning, China.
Front Nutr. 2022 Nov 15;9:976216. doi: 10.3389/fnut.2022.976216. eCollection 2022.
To explore the prognostic value of the preoperative neutrophil-albumin ratio (NAR) in patients with colorectal cancer (CRC) undergoing surgical treatment.
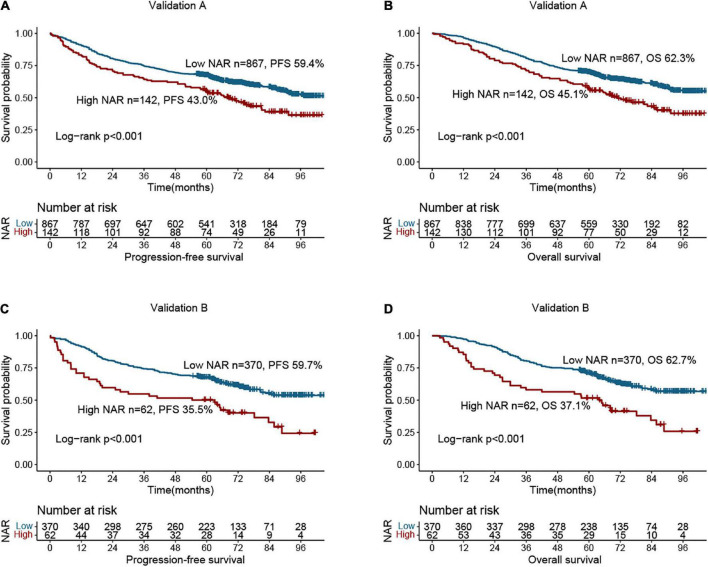
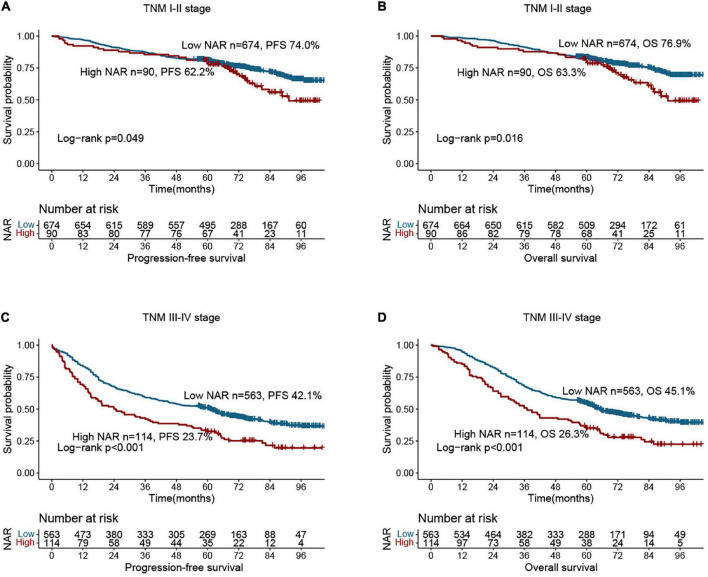
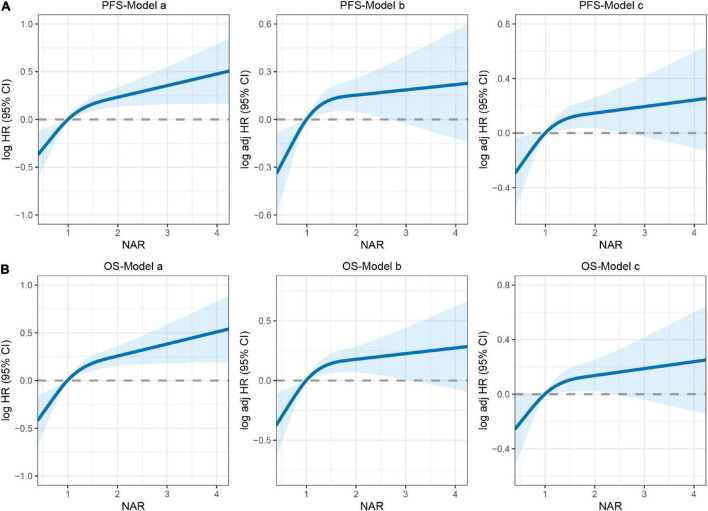
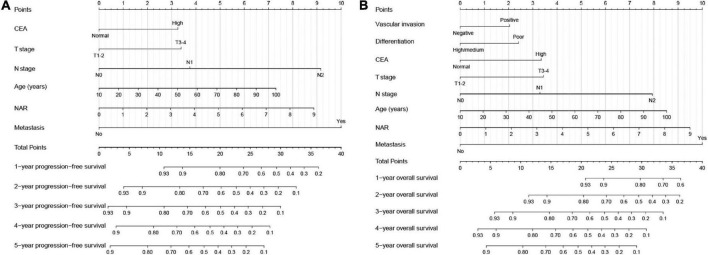
The standardized log-rank statistic was used to determine the optimal cut-off value for NAR. A logistic regression model was used to evaluate the value of NAR in predicting postoperative complications. Cox proportional hazards models were used to assess the independent association of NAR with progression-free survival (PFS) and overall survival (OS) in CRC patients. Restricted cubic splines were used to assess the relationship between continuous NAR and survival in CRC patients. The Kaplan-Meier method and log-rank test were used to compare survival differences between low and high NAR groups. NAR-based prognostic nomograms were constructed to predict the 1-5-year PFS and OS of CRC patients. The concordance index (C-index) and calibration curve were used to evaluate the prognostic accuracy of the nomograms.
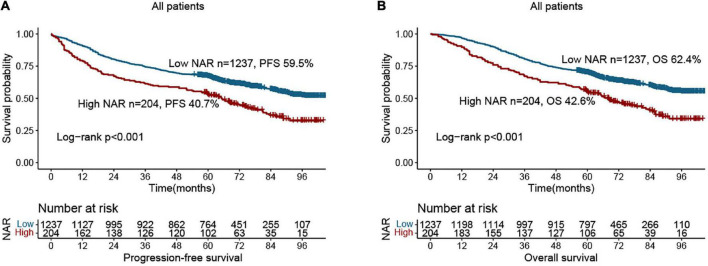
A total of 1,441 CRC patients were enrolled from January 2012 to December 2016. There were 904 men (62.7%) and 537 women (37.3%), with an average age of 58.12 ± 13.15 years. High NAR was closely associated with low BMI, advanced pathological stage, colon cancer, large tumors, vascular invasion, poor differentiation, high CEA levels, long hospital stay, and recurrence and metastasis. A high NAR was an independent risk factor for postoperative complications in CRC patients (OR: 2.298, 95% CI: 1.642-3.216, < 0.001). Patients with a high NAR had worse PFS (40.7 vs. 59.5%, < 0.001) and OS (42.6 vs. 62.4%, < 0.001). After adjusting for confounders, high NAR was independently associated with PFS (HR: 1.280, 95% CI: 1.031-1.589, = 0.025) and OS (HR: 1.280; 95% CI: 1.026-1.596, = 0.029) in CRC patients. The C-index and calibration curves showed that the NAR-based prognostic nomograms had good predictive accuracy.
High NAR was an independent risk factor for postoperative complications and long-term prognosis of CRC patients. NAR-based research could provide references for prognostic judgment and clinical decision-making of CRC patients.
探讨术前中性粒细胞与白蛋白比值(NAR)对接受手术治疗的结直肠癌(CRC)患者的预后价值。
采用标准化对数秩统计量确定NAR的最佳截断值。使用逻辑回归模型评估NAR在预测术后并发症方面的价值。采用Cox比例风险模型评估NAR与CRC患者无进展生存期(PFS)和总生存期(OS)的独立关联。使用受限立方样条评估CRC患者中连续NAR与生存之间的关系。采用Kaplan-Meier法和对数秩检验比较低NAR组和高NAR组之间的生存差异。构建基于NAR的预后列线图以预测CRC患者1至5年的PFS和OS。使用一致性指数(C指数)和校准曲线评估列线图的预后准确性。
2012年1月至2016年12月共纳入1441例CRC患者。其中男性904例(62.7%),女性537例(37.3%),平均年龄58.12±13.15岁。高NAR与低体重指数、晚期病理分期、结肠癌、大肿瘤、血管侵犯、低分化、高癌胚抗原水平、住院时间长以及复发和转移密切相关。高NAR是CRC患者术后并发症的独立危险因素(OR:2.298,95%CI:1.642 - 3.216,P<0.001)。高NAR患者的PFS(40.7%对59.5%,P<0.001)和OS(42.6%对62.4%,P<0.001)较差。在调整混杂因素后,高NAR与CRC患者的PFS(HR:1.280,95%CI:1.031 - 1.589,P = 0.025)和OS(HR:1.280;95%CI:1.026 - 1.596,P = 0.029)独立相关。C指数和校准曲线显示基于NAR的预后列线图具有良好的预测准确性。
高NAR是CRC患者术后并发症和长期预后的独立危险因素。基于NAR的研究可为CRC患者的预后判断和临床决策提供参考。