Coronary Heart Disease Center, Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Science and Peking Union Medical College, Beijing, China.
Medical Research and Biometrics Center, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Science and Peking Union Medical College, Beijing, China.
JAMA Netw Open. 2020 Oct 1;3(10):e2021677. doi: 10.1001/jamanetworkopen.2020.21677.
The incidence of acute myocardial infarction has increased over the past decades in China, and management challenges include an unbalanced economy, disparate resources, and variable access to medical care across the nation.
To examine the variations in care and outcomes of patients with ST-segment elevation myocardial infarction among 3 levels of hospitals in the typical Chinese public hospital model.
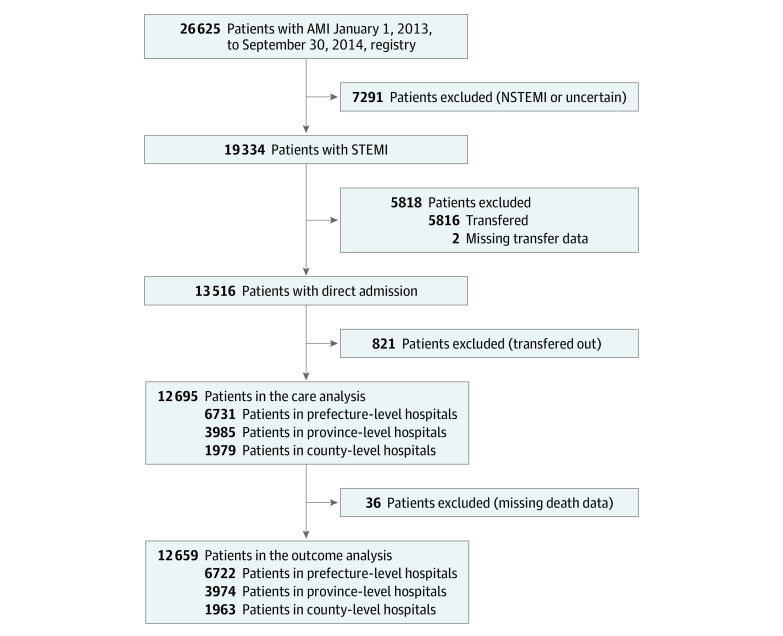
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study used data from the China Acute Myocardial Infarction Registry to compare the differences in care and outcomes among patients at 108 hospitals from 31 provinces and municipalities throughout mainland China. Participants included patients with ST-segment elevation myocardial infarction directly admitted to hospitals between January 2013 and September 2014. Data analyses were performed from June 2015 to June 2019.
Care in province-level, prefecture-level, or county-level hospitals in China.
The primary outcome was in-hospital mortality. Secondary outcomes included presentation, treatments, and major complications.
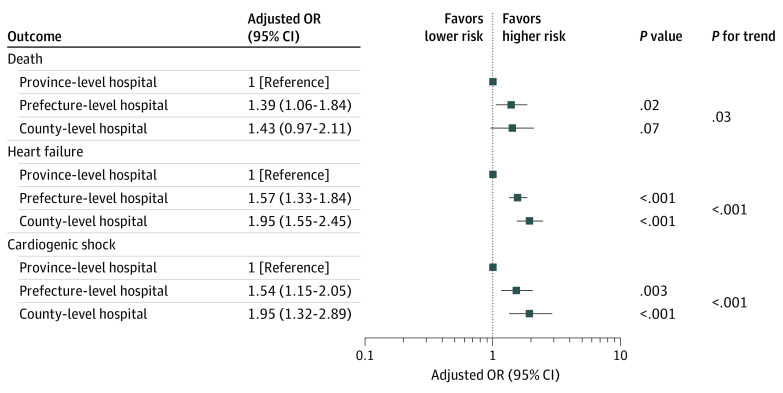
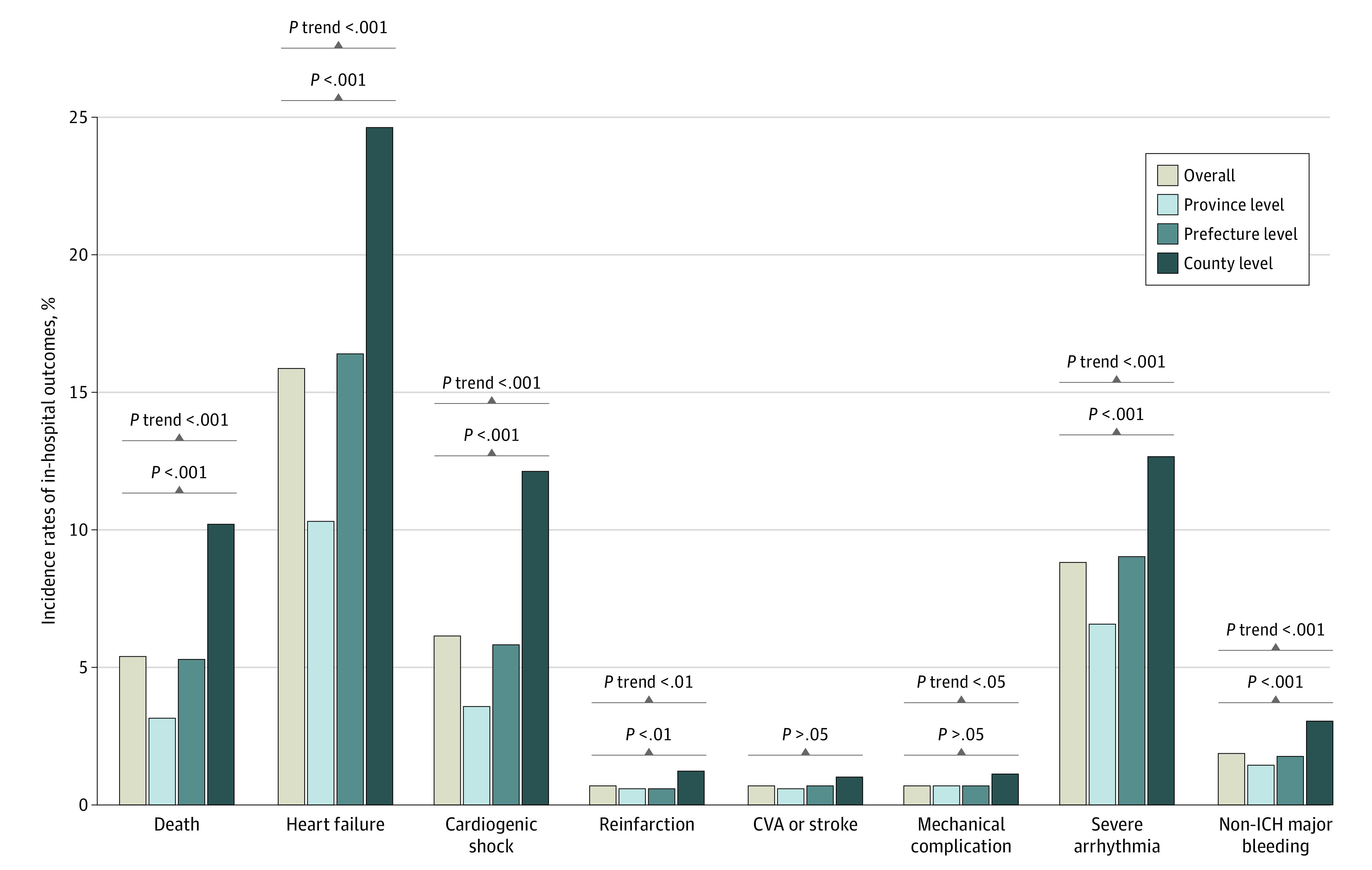
A total of 12 695 patients (9593 men [75.6%]; median [interquartile range] age, 63 [54-72] years) were included; 3985 were at province-level hospitals, 6731 were at prefecture-level hospitals, and 1979 were at county-level hospitals. Compared with patients admitted to province-level hospitals, those admitted to prefecture-level and county-level hospitals were older (median [interquartile range] age, 61 [52-70] years vs 63 [54-72] years and 65 [57-75] years) and more likely to be women (815 women [20.5%] vs 1620 women [24.1%] and 667 women [33.7%]). Patients in prefecture-level and county-level hospitals were less likely to use ambulances compared with patients at province-level hospitals (11.6% [95% CI, 10.8%-12.4%] and 12.0% [95% CI, 10.6%-13.5%] vs 19.4% [95% CI, 18.1%-20.7%]; P < .001) and were less likely to experience early presentation, with onset-to-arrival times less than 12 hours for 75.3% (95% CI, 73.9%-76.6%) of patients at province-level hospitals, 70.8% (95% CI, 69.7%-71.9%) of patients at prefecture-level hospitals, and 69.8% (95% CI, 67.7%-71.8%) of patients at county-level hospitals (P < .001). The rates of reperfusion therapy were significantly lower in low-level hospitals (54.3% [95% CI, 53.1%-55.5%] for prefecture-level hospitals and 45.8% [95% CI, 43.6%-48.1%] for county-level hospitals) compared with province-level hospitals (69.4% [95% CI, 67.9%-70.8%]; P < .001). There was a progressively higher rate of in-hospital mortality at the 3 levels of hospitals: 3.1% (95% CI, 2.6%-3.7%) for province-level hospitals, 5.3% (95% CI, 4.8%-5.9%) for prefecture-level hospitals, and 10.2% (95% CI, 8.9%-11.7%) for county-level hospitals (P for trend < .001). After adjustment for patient characteristics, presentation, hospital facility, and treatments, the odds of death remained higher in prefecture-level (odds ratio, 1.39 [95% CI, 1.06-1.84]) and county-level (odds ratio, 1.43 [95% CI, 0.97-2.11]) hospitals compared with province-level hospitals (P for trend = .04).
These findings suggest that there are significant variations in care and outcomes of patients among the 3 levels of hospitals in China. More efforts should be made to address the identified gaps, particularly in the prefecture-level and county-level hospitals. This work can inform national quality improvements efforts in China and in other developing countries.
过去几十年,中国急性心肌梗死的发病率有所上升,管理挑战包括经济不平衡、资源差异以及全国医疗服务获取的不平衡。
在典型的中国公立医院模式下,比较三级医院中 ST 段抬高型心肌梗死患者的治疗差异及结局。
设计、地点和参与者:本横断面研究使用了中国急性心肌梗死注册研究的数据,比较了中国大陆 31 个省、直辖市的 108 家医院直接收治的 ST 段抬高型心肌梗死患者之间的治疗差异和结局。参与者包括直接收治入院的 ST 段抬高型心肌梗死患者,纳入时间为 2013 年 1 月至 2014 年 9 月。数据分析于 2015 年 6 月至 2019 年 6 月进行。
中国省级、市级或县级医院的治疗。
主要结局是院内死亡率。次要结局包括发病情况、治疗和主要并发症。
共纳入 12695 例患者(9593 例男性[75.6%];中位数[四分位间距]年龄,63[54-72]岁),其中 3985 例来自省级医院,6731 例来自市级医院,1979 例来自县级医院。与省级医院相比,市级和县级医院的患者年龄更大(中位数[四分位间距]年龄,61[52-70]岁比 63[54-72]岁和 65[57-75]岁),女性患者比例更高(815 例女性[20.5%]比 1620 例女性[24.1%]和 667 例女性[33.7%])。与省级医院相比,市级和县级医院患者使用救护车的比例较低(11.6%[95%置信区间,10.8%-12.4%]和 12.0%[95%置信区间,10.6%-13.5%]比 19.4%[95%置信区间,18.1%-20.7%];P<0.001),且发病至就诊时间更晚,省级医院 75.3%(95%置信区间,73.9%-76.6%)的患者就诊时间在 12 小时以内,市级医院 70.8%(95%置信区间,69.7%-71.9%)的患者和县级医院 69.8%(95%置信区间,67.7%-71.8%)的患者就诊时间在 12 小时以内(P<0.001)。低级别医院的再灌注治疗率明显较低(市级医院 54.3%[95%置信区间,53.1%-55.5%]和县级医院 45.8%[95%置信区间,43.6%-48.1%]),与省级医院 69.4%(95%置信区间,67.9%-70.8%)相比,差异有统计学意义(P<0.001)。3 级医院的院内死亡率呈逐渐升高趋势:省级医院为 3.1%(95%置信区间,2.6%-3.7%),市级医院为 5.3%(95%置信区间,4.8%-5.9%),县级医院为 10.2%(95%置信区间,8.9%-11.7%)(P<0.001)。在调整了患者特征、发病情况、医院设施和治疗情况后,市级(比值比,1.39[95%置信区间,1.06-1.84])和县级(比值比,1.43[95%置信区间,0.97-2.11])医院的死亡风险仍高于省级医院(P<0.001)。
这些发现表明,中国 3 级医院之间在治疗和结局方面存在显著差异。应做出更多努力来解决这些差距,特别是在市级和县级医院。这项工作可以为中国和其他发展中国家的国家质量改进工作提供信息。