Department of Internal Medicine, University of New Mexico Health Sciences Center, Albuquerque, New Mexico, USA.
Division of Public Health, Department of Family and Preventative Medicine, University of Utah, Salt Lake City, UT, USA.
J Diabetes Complications. 2021 Feb;35(2):107753. doi: 10.1016/j.jdiacomp.2020.107753. Epub 2020 Oct 9.
Home-Based Kidney Care (HBKC) is a pragmatic treatment approach that addresses patient preferences and cultural barriers to healthcare. We previously reported the results of a clinical trial of HBKC vs. usual care in a cohort of Zuni Indians in New Mexico. This study investigated the potential for differential efficacy of HBKC vs. usual care according to type 2 diabetes (T2DM) status.
We analyzed the data from all individuals who participated in a randomized clinical trial that compared HBKC to usual care among patients with CKD, and assessed whether the effect of the HBKC intervention affected the subset of patients with T2DM differently than those individuals without T2DM. We used linear regression models to estimate the effect of HBKC on improvement in Patient Activation Measure (PAM) total scores within the groups of participants defined by T2DM status, and to compare the effects between these two groups. We used generalized estimating equations (GEE) to account for household clustering.
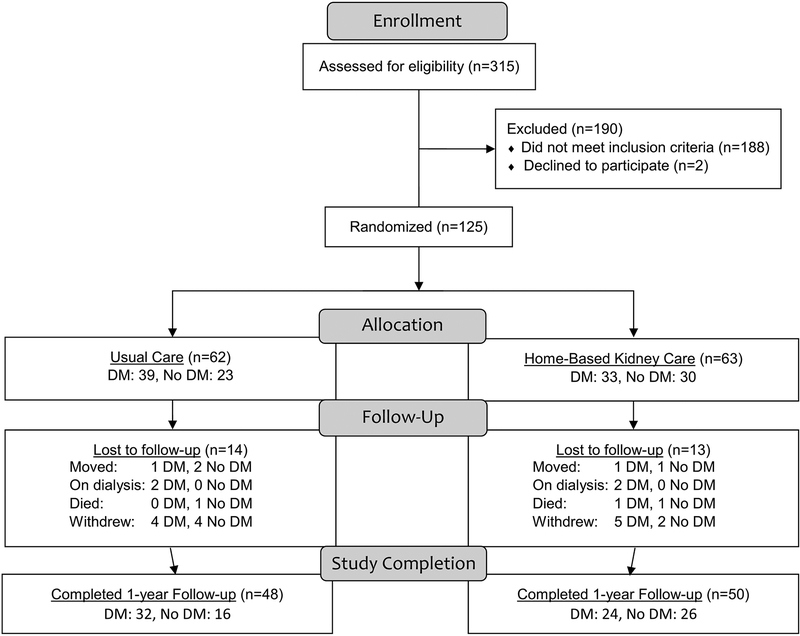
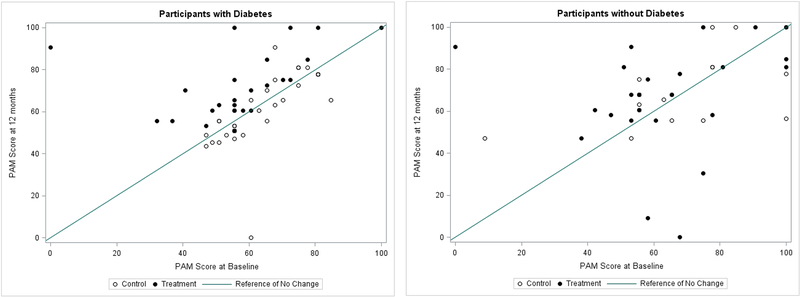
The original study enrolled 63 participants into the HBKC group, and 62 into the usual care. Ninety-eight of these individuals completed the 12-month intervention, 50 in the HBKC group and 48 in the usual care group. The present study compared the intervention effect in the 56 participants with T2DM (24 participants in the HBKC group and 32 in usual care) to the intervention effect in the 42 participants without T2DM (26 participants in the HBKC group and 16 in usual care). Those with T2DM who received the HBKC intervention experienced an average increase in PAM total scores of 16.0 points (95% Confidence Interval: 8.8-23.1) more than those with T2DM who were in the usual care group. For those without T2DM, the intervention had essentially no effect, with those who received the HBKC intervention having an average PAM total scores that was 1.4 points (95% C.I.: -12.4 to 9.6) lower than those who received usual care. There was a significantly different HBKC treatment effect by T2DM status (p = 0.02).
This secondary analysis suggests that the effectiveness of this HBKC intervention on increasing patient activation is most notable among those CKD patients who also have T2DM.
家庭肾脏护理(HBKC)是一种务实的治疗方法,可满足患者对医疗保健的偏好和文化障碍。我们之前报告了在新墨西哥州的祖尼印第安人中进行的 HBKC 与常规护理的临床试验结果。这项研究调查了 HBKC 与常规护理的疗效在 2 型糖尿病(T2DM)患者中的差异。
我们分析了所有参与比较慢性肾脏病患者 HBKC 与常规护理的随机临床试验的个体的数据,并评估了 HBKC 干预的效果是否会对 T2DM 亚组与非 T2DM 个体产生不同的影响。我们使用线性回归模型来估计 HBKC 对 PAM 总评分改善的影响,参与者根据 T2DM 状态分为两组,并比较这两组之间的效果。我们使用广义估计方程(GEE)来考虑家庭聚类。
原始研究将 63 名参与者纳入 HBKC 组,62 名纳入常规护理组。其中 98 名完成了 12 个月的干预,HBKC 组 50 名,常规护理组 48 名。本研究将 56 名 T2DM 患者(HBKC 组 24 名,常规护理组 32 名)的干预效果与 42 名非 T2DM 患者(HBKC 组 26 名,常规护理组 16 名)的干预效果进行了比较。接受 HBKC 干预的 T2DM 患者 PAM 总评分平均增加 16.0 分(95%置信区间:8.8-23.1),高于接受常规护理组的患者。对于没有 T2DM 的患者,干预几乎没有效果,接受 HBKC 干预的患者 PAM 总评分平均比接受常规护理的患者低 1.4 分(95%置信区间:-12.4 至 9.6)。T2DM 状态的 HBKC 治疗效果存在显著差异(p=0.02)。
这项二次分析表明,HBKC 干预对提高患者积极性的有效性在同时患有 CKD 和 T2DM 的患者中最为显著。