Noh Jeong-Eun, Oh Seung-Hun, Park In-Hyun, Song Jihwan
Department of Biomedical Science, CHA Stem Cell Institute, CHA University, Seongnam-si, South Korea.
Department of Neurology, CHA Bundang Medical Center, CHA University, Seongnam-si, South Korea.
Front Cell Neurosci. 2020 Sep 25;14:546659. doi: 10.3389/fncel.2020.546659. eCollection 2020.
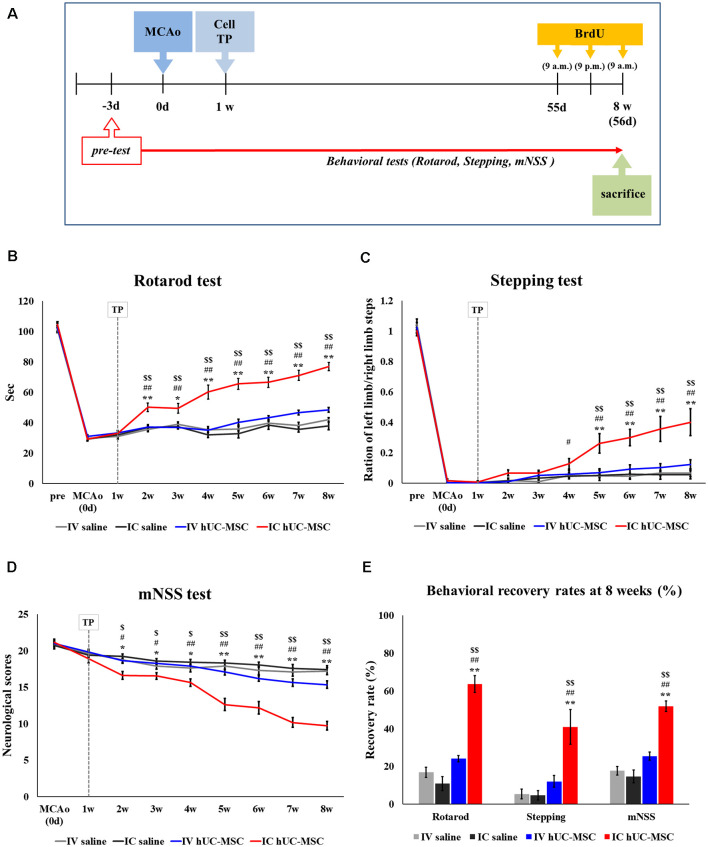
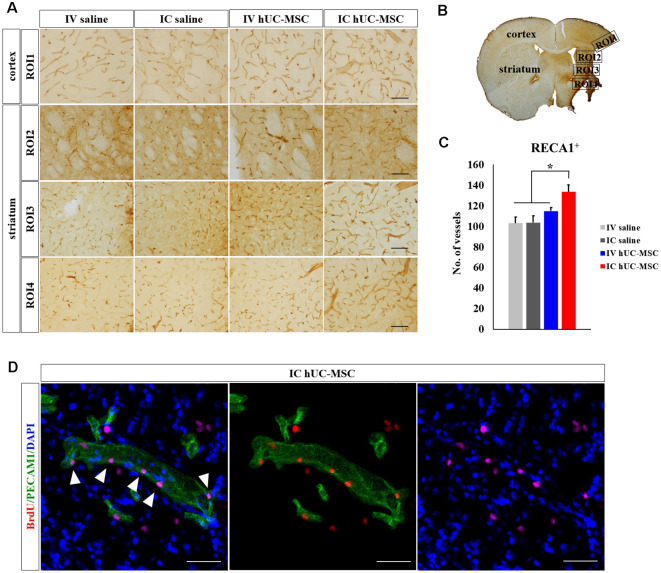
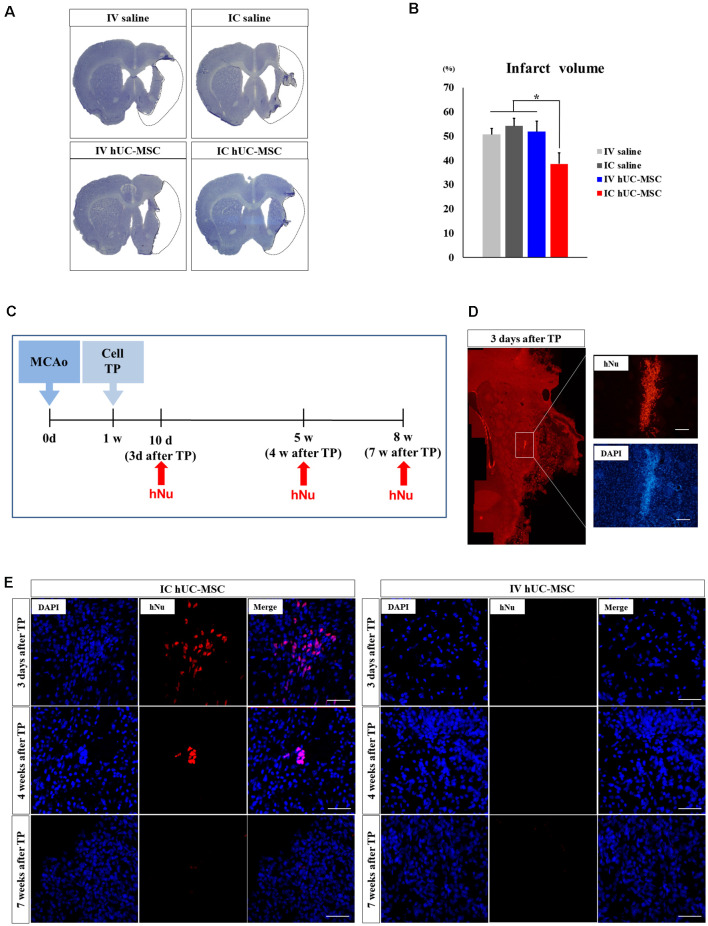
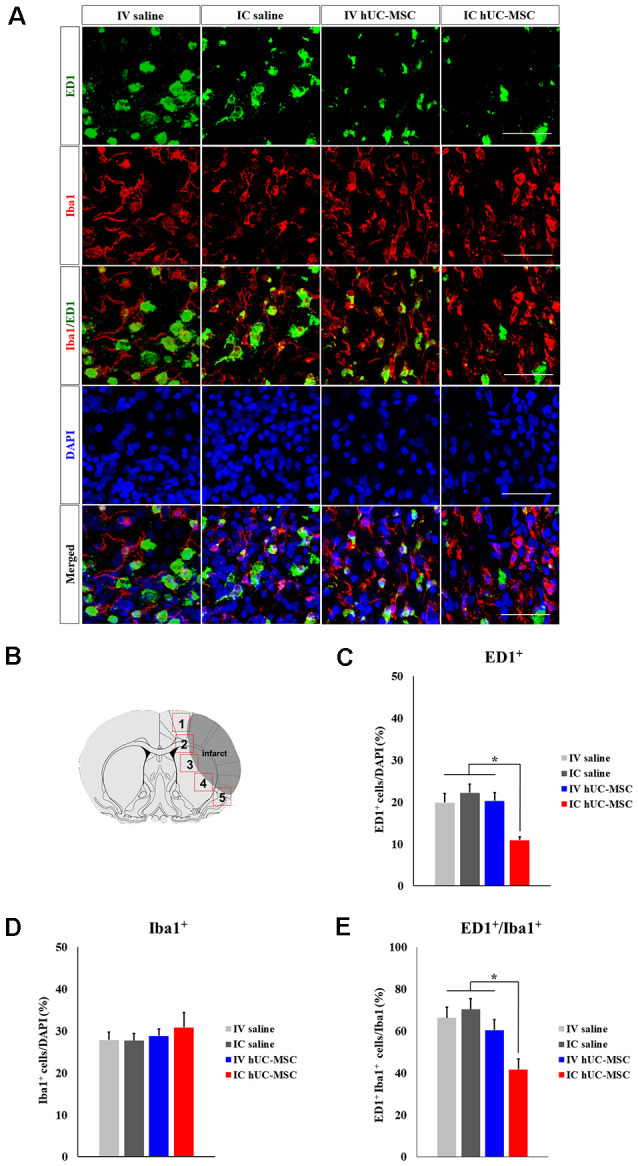
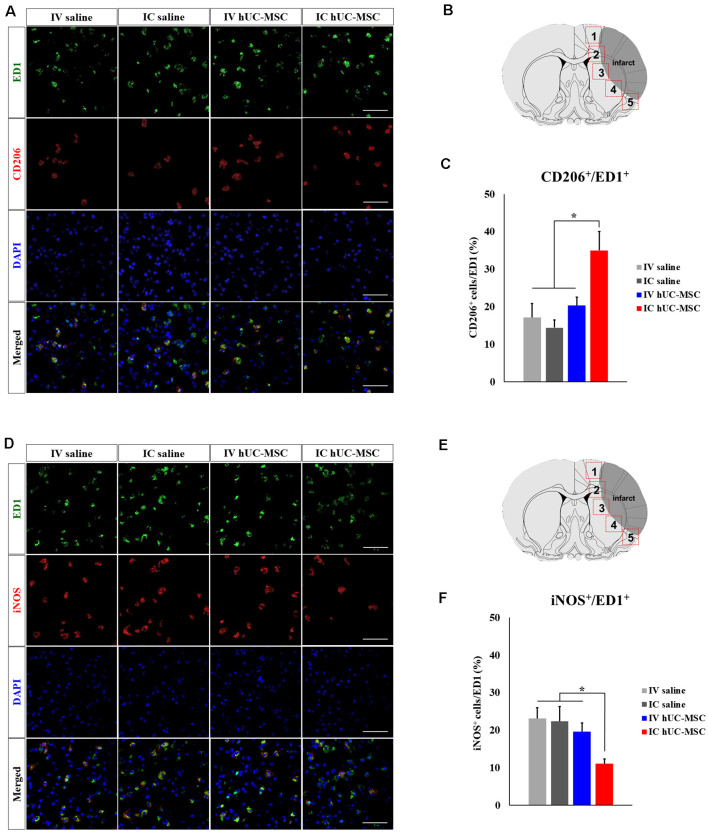
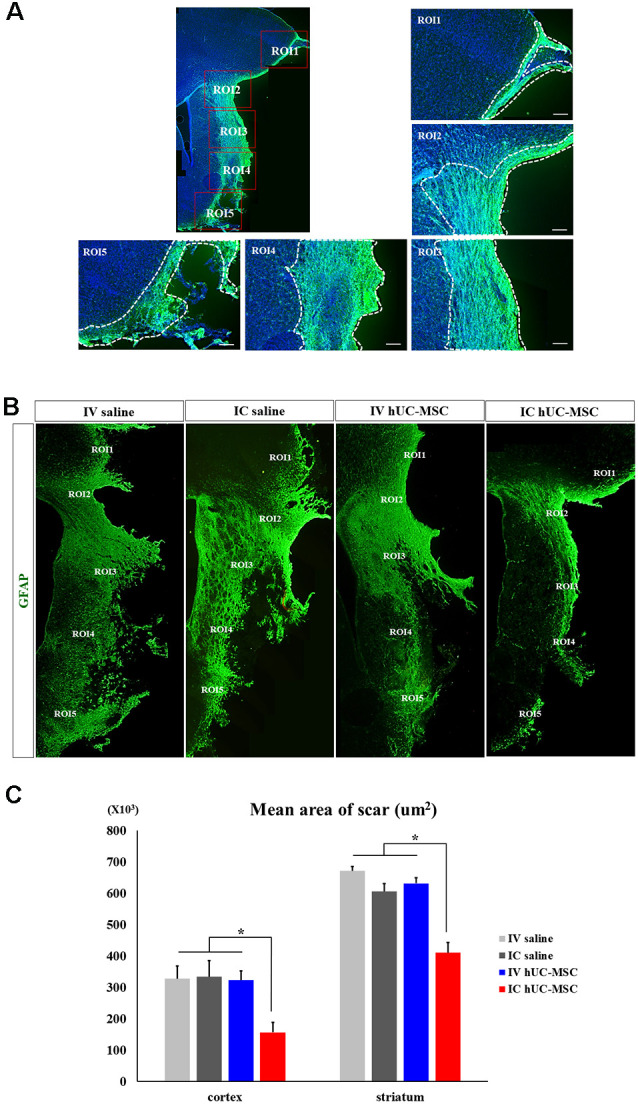
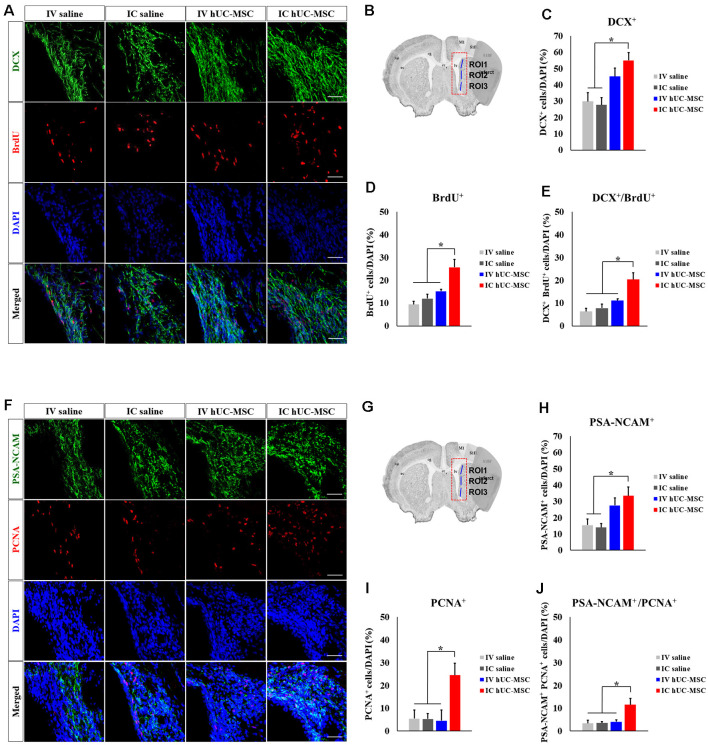
In subacute and chronic phases of the stroke, there are no therapeutics available at present to promote functional recovery. Human umbilical cord-derived mesenchymal stromal cells (hUC-MSCs) are one of the candidate cell types for treating subacute-phase stroke. The benefits of cell-based therapy largely depend on the migratory capacity of products administered, as well as their potential for engraftment in targeted tissues and paracrine activities. Timing and delivery modes may also influence the outcomes of stem-cell therapy. Still, the functional recuperative effects of differing hUC-MSC delivery modes, about cell replacement and cell-to-cell paracrine activity levels, have yet to be clarified in subacute phases of stroke.This study was conducted to compare the therapeutic effects of various delivery routes when administering Good Manufacturing Practice (GMP)-grade hUC-MSCs in a rodent model of subacute-phase stroke. Cell aliquots (1 × 10) were given to rats as intravenous (IV) injections or intracerebral (IC) transplants 1 week after middle cerebral artery occlusion (MCAo). Transplanted rats were examined up to 7 weeks later using various behavioral tests and immunohistochemical analyses. Most IC-transplanted cells survived for short periods (i.e., <4 weeks after receipt) and gradually disappeared, whereas IV-injected cells were undetectable in the brain at the same time points (i.e., 3 days, 4 weeks, or 7 weeks after injection). Although short-lived, IC-transplanted cells effectively improved behavioral deficits, serving to reduce infarct volumes and glial scar formation, increase subventricular counts of proliferating neuroblasts, and promote cerebrovascular ingrowth in ischemic penumbra regions. IV injection, however, failed to improve behavioral function or histologic parameters during the same 7-week time frame. These findings overall suggest that IC transplantation is preferable to IV injection for delivery of hUC-MSCs during subacute phases of stroke.
在中风的亚急性期和慢性期,目前尚无促进功能恢复的治疗方法。人脐带间充质基质细胞(hUC-MSCs)是治疗亚急性期中风的候选细胞类型之一。基于细胞的治疗的益处很大程度上取决于所施用产品的迁移能力,以及它们在靶组织中的植入潜力和旁分泌活性。时间和递送方式也可能影响干细胞治疗的结果。然而,在中风亚急性期,不同hUC-MSC递送方式在细胞替代和细胞间旁分泌活性水平方面的功能恢复效果尚未明确。本研究旨在比较在亚急性期中风的啮齿动物模型中给予药品生产质量管理规范(GMP)级hUC-MSCs时各种递送途径的治疗效果。在大脑中动脉闭塞(MCAo)1周后,将细胞等分试样(1×10)静脉内(IV)注射或脑内(IC)移植给大鼠。在长达7周后,使用各种行为测试和免疫组织化学分析对移植大鼠进行检查。大多数IC移植细胞存活时间较短(即接受后<4周)并逐渐消失,而在相同时间点(即注射后3天、4周或7周)在大脑中未检测到IV注射的细胞。尽管IC移植细胞寿命短暂,但能有效改善行为缺陷,减少梗死体积和胶质瘢痕形成,增加增殖神经母细胞的脑室下计数,并促进缺血半暗带区域的脑血管向内生长。然而,在相同的7周时间内,IV注射未能改善行为功能或组织学参数。这些发现总体表明,在中风亚急性期,IC移植比IV注射更适合递送hUC-MSCs。