College of Natural, Applied, and Health Sciences, Kean University, Union, New Jersey, USA.
Center for Discovery and Innovation, The John Theurer Cancer Center, Hackensack-Meridian Health, Nutley, New Jersey, USA.
Cancer Rep (Hoboken). 2021 Apr;4(2):e1311. doi: 10.1002/cnr2.1311. Epub 2020 Oct 26.
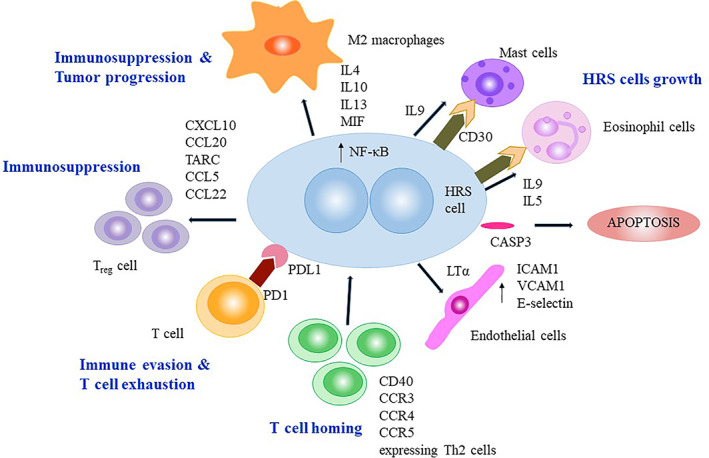
Classical Hodgkin lymphoma (cHL) is a unique lymphoid malignancy with a tumor microenvironment (TME) consisting of a small number of neoplastic-Hodgkin and Reed-Sternberg (H-RS) cells (<1%), surrounded by a large number of nonneoplastic infiltrating immune cells (>90%). The TME of cHL critically depends on immune cells to support tumor growth as H-RS cells cannot survive and proliferate in isolation.
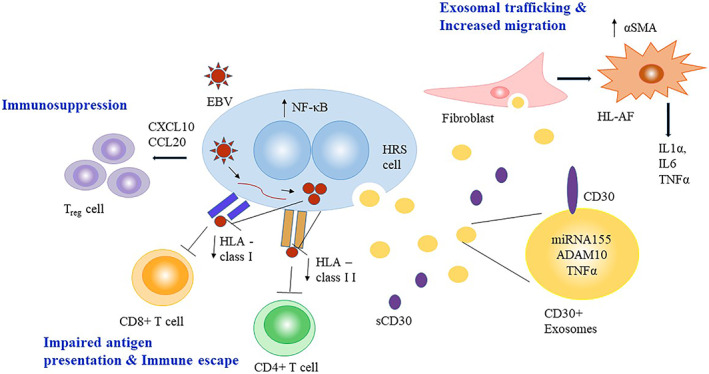
Programmed cell death protein 1 (PD-1) ligand expressed on H-RS cells inhibits the clearance of tumor by causing T-cell exhaustion. Nivolumab and pembrolizumab, PD-1 inhibitors, have been proven to be effective in treating adult and pediatric patients with R/R cHL. Tumor-associated macrophages (TAMs) are a central component of TME and are known to cause poor prognosis in adult HL. However, the prognostic impact of CD68+ TAMs in pediatric HL remains ambiguous. EBV modulates the tumor milieu of HL and plays a strategic role in immune escape by enrichment of the TME with T cells and associated immunosuppressive cytokines in adult HL. In contrast, EBV+ pediatric patients have increased infiltration of CD8 T-cells and show a better therapeutic response suggesting viral-related TME is distinct in childhood HL. The role of CASP3 in apoptosis of H-RS cells and its correlation with response prediction in adult and pediatric HL suggest it may serve as a potential biomarker. In cHL, CD30, EBV, and NF-κB signaling employ exosomes for cell-cell communication that triggers the migration capacity of fibroblasts, stimulate to produce proinflammatory cytokines, and help to create a tumor-supportive microenvironment.
The cHL microenvironment is distinct in adult and pediatric HL. Future studies are required to understand the role of interplay between H-RS cells and EBV-associated microenvironment and their clinical outcome. They may present novel therapeutic targets for the development of antilymphoma therapy.
经典型霍奇金淋巴瘤(cHL)是一种独特的淋巴恶性肿瘤,其肿瘤微环境(TME)由少数肿瘤性霍奇金和里斯-斯滕伯格(H-RS)细胞组成(<1%),周围是大量非肿瘤性浸润免疫细胞(>90%)。cHL 的 TME 严重依赖免疫细胞来支持肿瘤生长,因为 H-RS 细胞不能孤立存活和增殖。
H-RS 细胞表达的程序性细胞死亡蛋白 1(PD-1)配体导致 T 细胞耗竭,从而抑制肿瘤的清除。PD-1 抑制剂纳武单抗和帕博利珠单抗已被证明可有效治疗成人和儿科复发/难治性 cHL 患者。肿瘤相关巨噬细胞(TAMs)是 TME 的核心组成部分,已知其导致成人 HL 预后不良。然而,CD68+TAMs 在儿科 HL 中的预后影响仍存在争议。EBV 调节 HL 的肿瘤微环境,并通过在成人 HL 中丰富 TME 中的 T 细胞和相关免疫抑制细胞因子,在免疫逃逸中发挥战略作用。相比之下,EBV+儿科患者 CD8 T 细胞浸润增加,并表现出更好的治疗反应,表明儿童 HL 中的病毒相关 TME 是不同的。CASP3 在 H-RS 细胞凋亡中的作用及其与成人和儿科 HL 反应预测的相关性表明,它可能作为一种潜在的生物标志物。在 cHL 中,CD30、EBV 和 NF-κB 信号通路利用外泌体进行细胞间通讯,触发成纤维细胞的迁移能力,刺激产生促炎细胞因子,并有助于创建肿瘤支持的微环境。
cHL 的微环境在成人和儿科 HL 中是不同的。需要进一步研究以了解 H-RS 细胞与 EBV 相关微环境之间相互作用及其临床结果的作用。它们可能为开发抗淋巴瘤治疗提供新的治疗靶点。