Division of Endocrinology and Diabetes, Department of Internal Medicine I, University Hospital, University of Würzburg, Würzburg, Germany.
Central Laboratory, Core Unit Clinical Mass Spectrometry, University Hospital Würzburg, Würzburg, Germany.
Eur J Endocrinol. 2021 Jan;184(1):167-178. doi: 10.1530/EJE-20-0073.
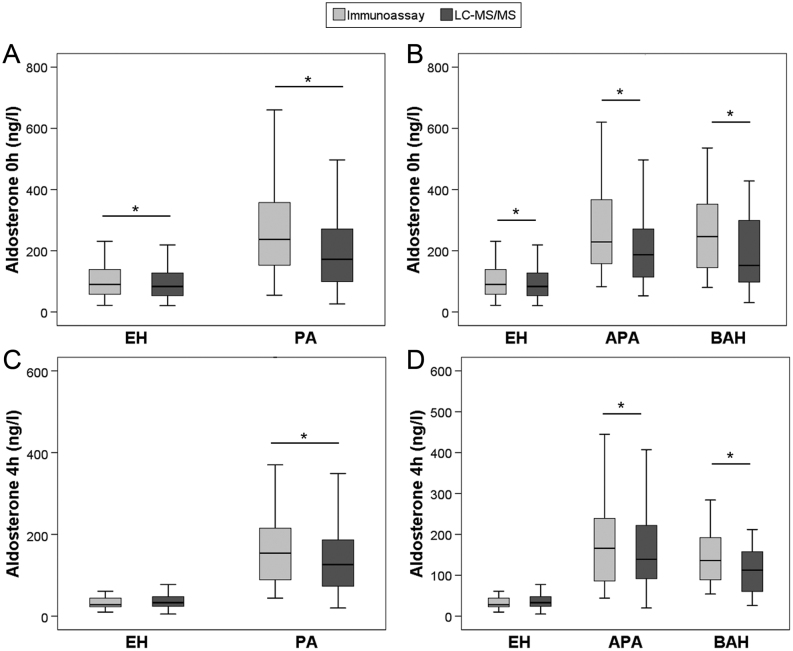
Saline infusion testing (SIT) for confirmation of primary aldosteronism (PA) is based on impaired aldosterone suppression in PA compared to essential hypertension (EH). In the past, aldosterone was quantified using immunoassays (IA). Liquid chromatography tandem mass spectrometry (LC-MS/MS) is increasingly used in clinical routine. We aimed at a method-specific aldosterone threshold for the diagnosis of PA during SIT and explored the diagnostic utility of steroid panel analysis.
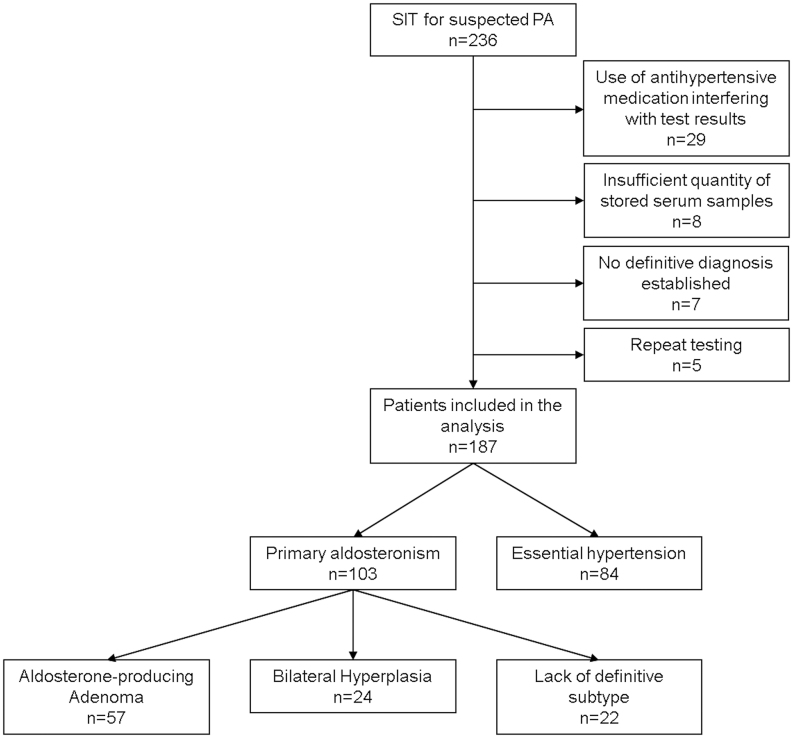
Retrospective cohort study of 187 paired SIT samples (2009-2018). Diagnosis of PA (n = 103) and EH (n = 84) was established based on clinical routine workup without using LC-MS/MS values.
Tertiary care center.
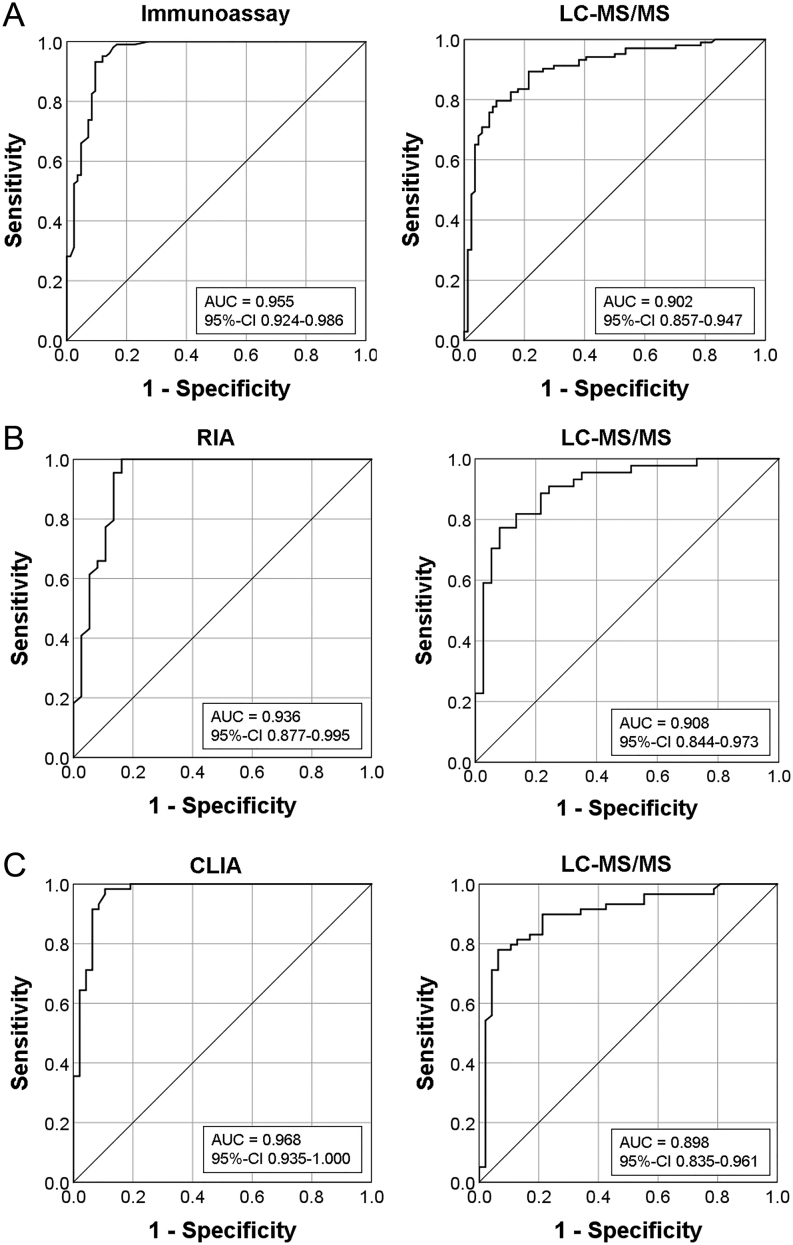
LC-MS/MS using a commercial steroid panel. Receiver operator characteristics analysis was used to determine method-specific cut-offs using a positive predictive value (PPV) of 90% as criterion.
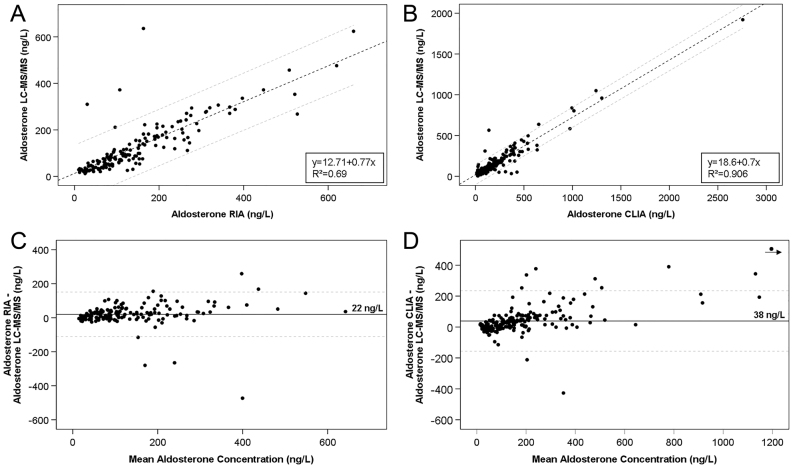
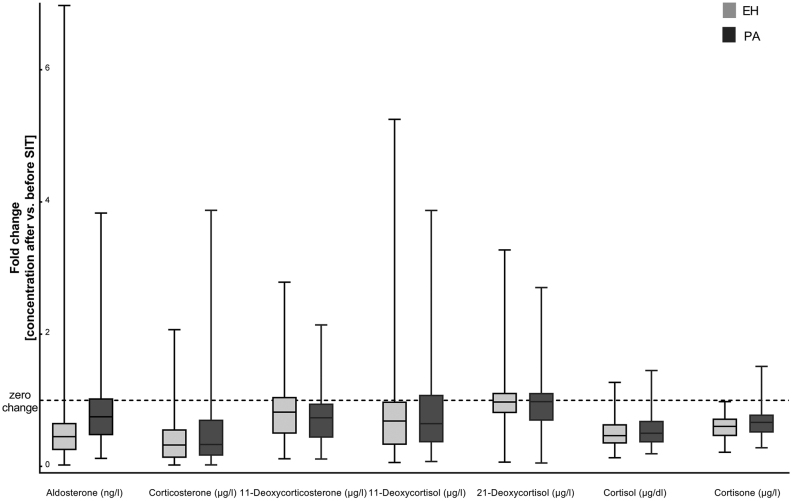
Aldosterone measured by IA was on average 31 ng/L higher than with LC-MS/MS. The cut-offs for PA confirmation were 54 ng/L for IA (sensitivity: 95%, 95% CI: 89.0-98.4; specificity: 87%, 95% CI: 77.8-93.3; area under the curve (AUC): 0.955, 95% CI: 0.924-0.986; PPV: 90%, 95% CI: 83.7-93.9) and 69 ng/L for LC-MS/MS (79%, 95% CI: 69.5-86.1; 89%, 95% CI: 80.6-95.0; 0.902, 95% CI: 0.857-0.947; 90%, 95% CI: 82.8-94.4). Other steroids did not improve SIT.
Aldosterone quantification with LC-MS/MS and IA yields comparable SIT-cut-offs. Lower AUC for LC-MS/MS is likely due to the spectrum of disease in PA and previous decision making based on IA results. Until data of a prospective trial with clinical endpoints are available, the suggested cut-off can be used in clinical routine.
盐水输注试验(SIT)用于原发性醛固酮增多症(PA)的确认,其依据是与原发性高血压(EH)相比,PA 患者的醛固酮抑制作用受损。过去,醛固酮的定量检测使用免疫测定法(IA)。液相色谱串联质谱法(LC-MS/MS)在临床常规中越来越多地被使用。我们旨在确定 SIT 期间用于诊断 PA 的特定方法的醛固酮阈值,并探讨类固醇谱分析的诊断效用。
2009 年至 2018 年期间对 187 对 SIT 样本进行的回顾性队列研究。根据临床常规评估确定 PA(n=103)和 EH(n=84)的诊断,未使用 LC-MS/MS 值。
三级护理中心。
使用商业类固醇谱的 LC-MS/MS。使用阳性预测值(PPV)为 90%作为标准的接收器工作特性分析,确定特定方法的截止值。
IA 测量的醛固酮平均比 LC-MS/MS 高 31ng/L。PA 确认的截止值为 IA 54ng/L(敏感性:95%,95%CI:89.0-98.4;特异性:87%,95%CI:77.8-93.3;曲线下面积(AUC):0.955,95%CI:0.924-0.986;PPV:90%,95%CI:83.7-93.9)和 LC-MS/MS 的 69ng/L(79%,95%CI:69.5-86.1;89%,95%CI:80.6-95.0;0.902,95%CI:0.857-0.947;90%,95%CI:82.8-94.4)。其他类固醇并未改善 SIT。
使用 LC-MS/MS 和 IA 进行的醛固酮定量检测可产生可比的 SIT 截止值。LC-MS/MS 的 AUC 较低可能是由于 PA 疾病谱和基于 IA 结果的先前决策。在具有临床终点的前瞻性试验数据可用之前,建议的截止值可用于临床常规。