Department of Medicine III, University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany.
Institute of Clinical Chemistry and Laboratory Medicine, University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany.
J Clin Endocrinol Metab. 2022 Apr 19;107(5):e2027-e2036. doi: 10.1210/clinem/dgab924.
Diagnosis of primary aldosteronism (PA) for many patients depends on positive results for the saline infusion test (SIT). Plasma aldosterone is often measured by immunoassays, which can return inaccurate results.
This study aimed to establish whether differences in aldosterone measurements by immunoassay versus mass spectrometry (MS) might impact confirmatory testing for PA.
This study, involving 240 patients tested using the SIT at 5 tertiary care centers, assessed discordance between immunoassay and MS-based measurements of plasma aldosterone.
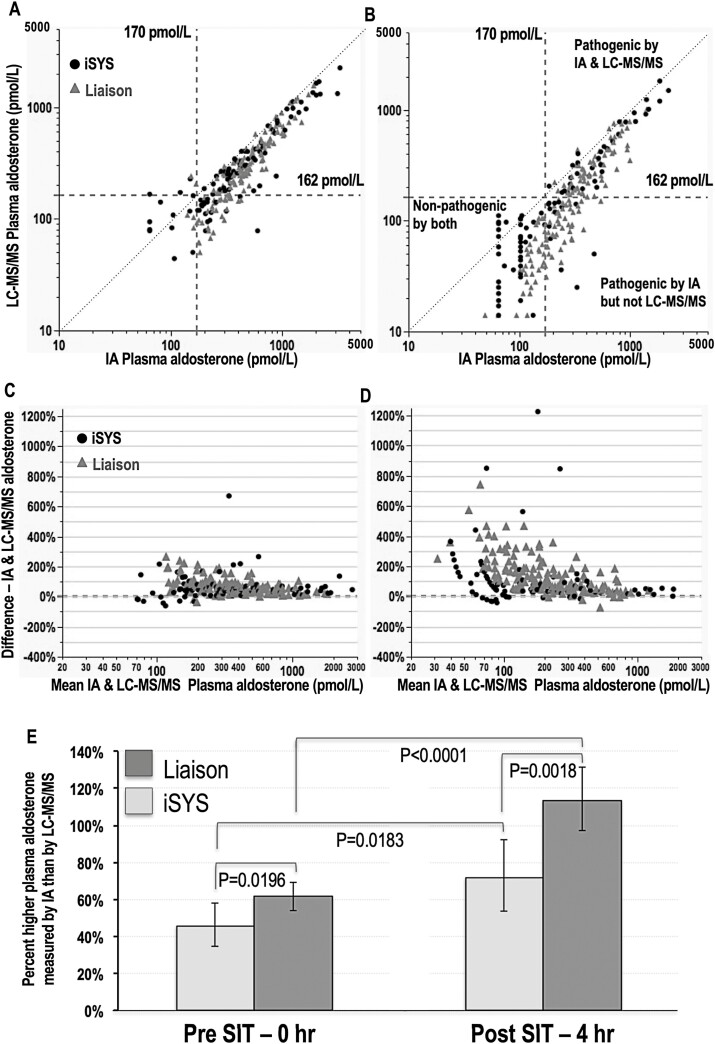
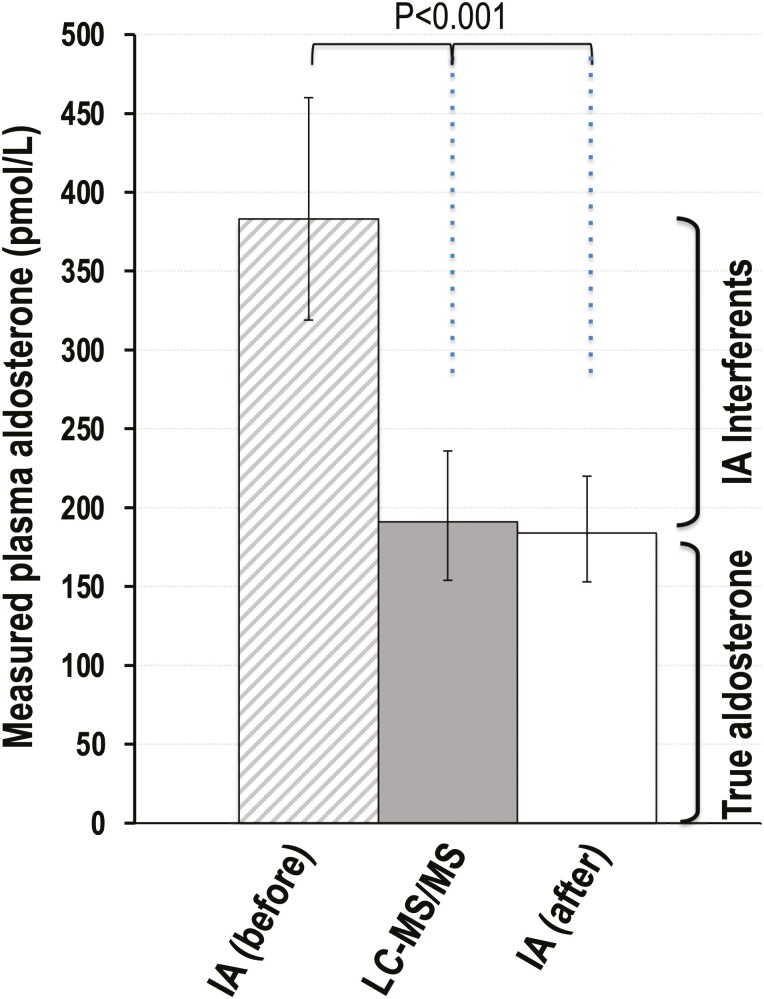
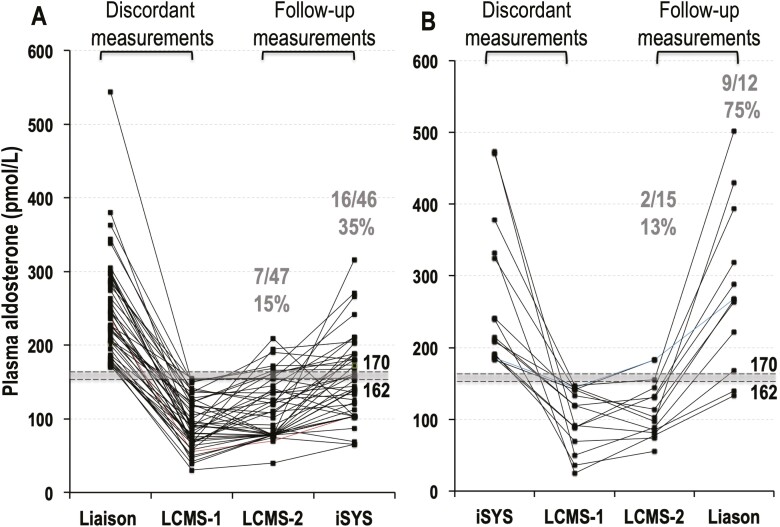
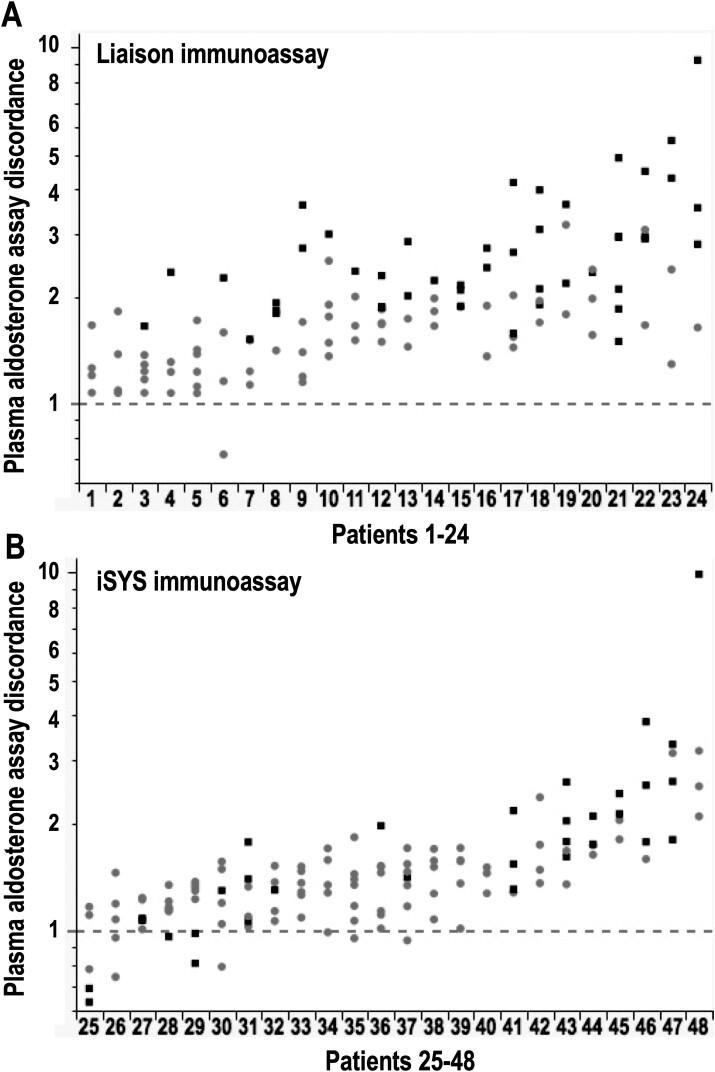
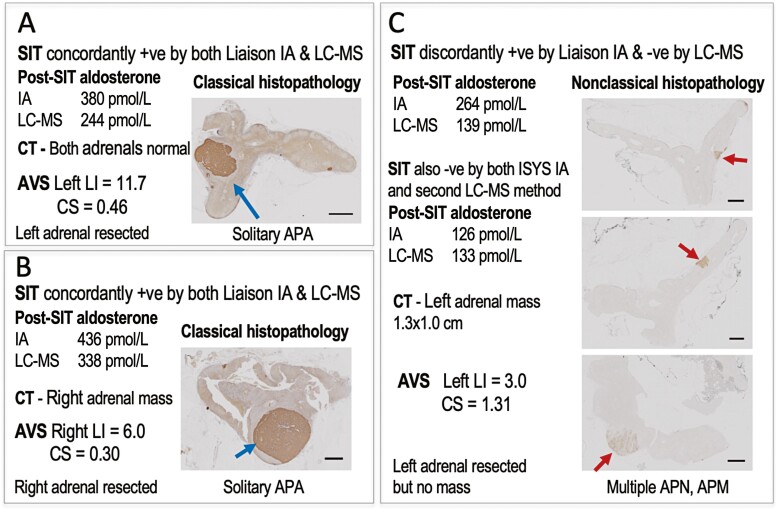
Plasma aldosterone measured by Liaison and iSYS immunoassays were respectively 86% and 58% higher than determined by MS. With an immunoassay-based SIT cutoff for aldosterone of 170 pmol/L, 78 and 162 patients had, respectivel, negative and positive results. All former patients had MS-based measurements of aldosterone < 117 pmol/L, below MS-based cutoffs of 162 pmol/L. Among the 162 patients with pathogenic SIT results, MS returned nonpathologic results in 62, including 32 under 117 pmol/L. Repeat measurements by an independent MS method confirmed nonpathogenic results in 53 patients with discordant results. Patients with discordant results showed a higher (P < 0.0001) prevalence of nonlateralized than lateralized adrenal aldosterone production than patients with concordant results (83% vs 28%). Among patients with nonlateralized aldosterone production, 66% had discordant results. Discordance was more prevalent for the Liaison than iSYS immunoassay (32% vs 16%; P = 0.0065) and was eliminated by plasma purification to remove interferents.
These findings raise concerns about the validity of immunoassay-based diagnosis of PA in over 60% of patients with presumed bilateral disease. We provide a simple solution to minimize immunoassay inaccuracy-associated misdiagnosis of PA.
许多原发性醛固酮增多症(PA)患者的诊断依赖于盐水输注试验(SIT)的阳性结果。醛固酮的检测通常采用免疫测定法,但这种方法可能会得出不准确的结果。
本研究旨在确定免疫测定法与质谱法(MS)测量的醛固酮之间的差异是否会影响对 PA 的确诊性检测。
本研究纳入了在 5 家三级护理中心接受 SIT 检测的 240 名患者,评估了免疫测定法和 MS 检测的血浆醛固酮之间的差异。
Liaison 和 iSYS 免疫测定法检测的血浆醛固酮分别比 MS 法高 86%和 58%。采用基于免疫测定法的 SIT 截断值为 170 pmol/L,分别有 78 名和 162 名患者的结果分别为阴性和阳性。前者所有患者的 MS 法检测的醛固酮均<117 pmol/L,低于 MS 法的截断值 162 pmol/L。在 162 名有致病性 SIT 结果的患者中,MS 法返回非致病性结果的有 62 例,其中 32 例<117 pmol/L。采用独立的 MS 方法进行重复测量,在结果不一致的 53 例患者中确认了非致病性结果。结果不一致的患者比结果一致的患者(83%比 28%)更普遍地表现出非优势侧肾上腺醛固酮生成(P<0.0001)。在非优势侧醛固酮生成的患者中,66%的患者结果不一致。Liaison 免疫测定法比 iSYS 免疫测定法(32%比 16%;P=0.0065)更易出现不一致的结果,且通过去除干扰物的血浆净化可以消除这种不一致。
这些发现引起了人们对基于免疫测定法诊断 PA 的有效性的担忧,因为超过 60%的疑似双侧疾病患者可能会出现错误诊断。我们提供了一个简单的解决方案,以最大程度地减少因免疫测定法不准确而导致的 PA 误诊。