Department of Clinical Sciences, Lund University, Malmö, Sweden.
Vascular Center, Department of Cardiothoracic and Vascular Surgery, Skåne University Hospital, Malmö, Sweden.
Scand J Surg. 2021 Jun;110(2):123-129. doi: 10.1177/1457496920969084. Epub 2020 Oct 29.
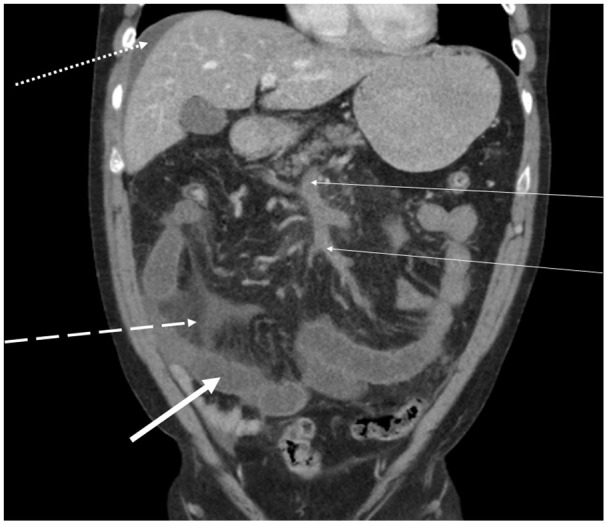
Acute mesenteric venous thrombosis accounts for up to 20% of all patients with acute mesenteric ischemia in high-income countries. Acute mesenteric venous thrombosis is nowadays relatively more often diagnosed with intravenous contrast-enhanced computed tomography in the portal phase than at explorative laparotomy No high-quality comparative studies between anticoagulation alone, endovascular therapy, or surgery exists. The aim of the present systematic review was to offer a contemporary overview on management.
Eleven relevant published original studies with series of at least ten patients were retrieved from a Pub Med search between 2015 and 2020 using the Medical Subject Heading term "mesenteric venous thrombosis."
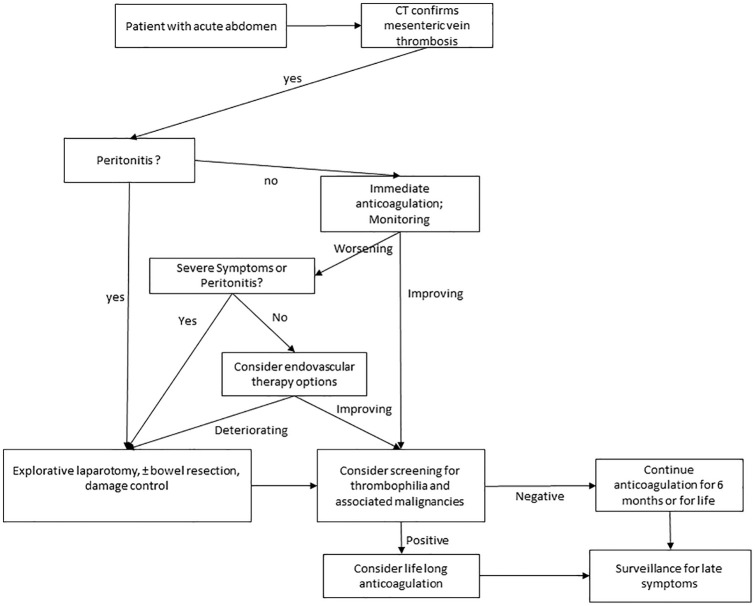
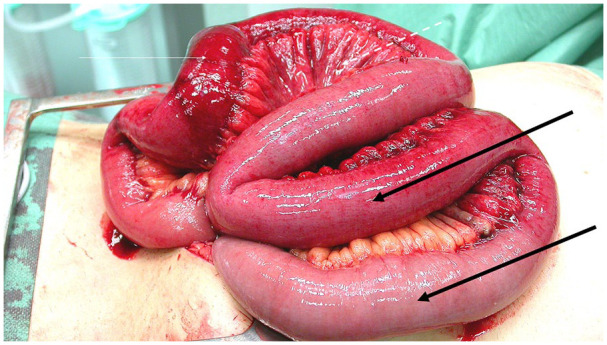
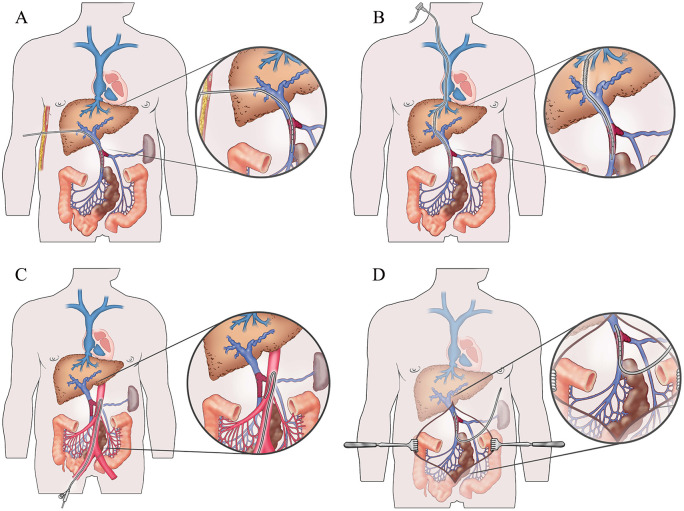
When MVT is diagnosed early, immediate anticoagulation with either unfractionated heparin or subcutaneous low-molecular-weight heparin should commence. Surgeons need to be aware of the importance to scrutinize the computed tomography images themselves for assessment of secondary intestinal abnormalities to mesenteric venous thrombosis and the risk of bowel resection and worse prognosis. Progression toward peritonitis is an indication for explorative laparotomy and assessment of bowel viability. Frank transmural small bowel necrosis should be resected and bowel anastomosis may be delayed for several days until second look. Meanwhile, intravenous full-dose unfractionated heparin should be given at the end of the first operation. Postoperative major intra-abdominal or gastrointestinal bleeding occurs rarely, but the heparin effect can instantaneously be reversed by . Patients who do not improve during conservative therapy with anticoagulation alone but without developing peritonitis may be subjected to endovascular therapy in expert centers. When the patient's intestinal function has recovered, with or without bowel resection, switch from parenteral unfractionated heparin or low-molecular-weight heparin therapy to oral anticoagulation can be performed. There is a trend that direct oral anticoagulants are increasingly used instead of vitamin K antagonists. Up to now, direct oral anticoagulants have been shown to be equally effective with the same rate of bleeding complications. Patients with no strong permanent trigger factor for mesenteric venous thrombosis such as intra-abdominal cancer should undergo blood screening for inherited and acquired thrombophilia.
Early diagnosis with emergency computed tomography with intravenous contrast-enhancement and imaging in the portal phase and anticoagulation therapy is necessary to be able to have a succesful non-operative succesful course.
在高收入国家,急性肠系膜静脉血栓形成占所有急性肠系膜缺血患者的 20%。如今,与剖腹探查术相比,经静脉注射对比剂增强门静脉期 CT 诊断急性肠系膜静脉血栓形成的情况更为常见。目前尚无单独抗凝、血管内治疗或手术治疗的高质量对比研究。本系统综述的目的是提供当前的治疗概况。
通过 2015 年至 2020 年在 Pub Med 上使用医学主题词“肠系膜静脉血栓形成”进行搜索,检索到 11 项至少包含 10 例患者的相关已发表原始研究系列。
当 MVT 早期诊断时,应立即开始使用普通肝素或皮下低分子量肝素进行抗凝治疗。外科医生需要注意仔细审查 CT 图像本身,以评估肠系膜静脉血栓形成的继发性肠道异常、肠切除和预后不良的风险。向腹膜炎进展是剖腹探查和肠活力评估的指征。明确的透壁性小肠坏死应切除,肠吻合术可延迟数天,直至二次探查。同时,在第一次手术后应给予静脉内全剂量普通肝素。术后主要腹腔或胃肠道出血很少见,但可通过鱼精蛋白迅速逆转肝素作用。对于单独抗凝治疗无改善但未发生腹膜炎的患者,可在专家中心进行血管内治疗。当患者的肠道功能恢复后,无论是否进行肠切除,都可以从静脉注射普通肝素或低分子量肝素治疗转为口服抗凝治疗。越来越多的趋势是使用直接口服抗凝剂而不是维生素 K 拮抗剂。到目前为止,直接口服抗凝剂与出血并发症发生率相同,同样有效。对于没有腹腔内癌症等强烈永久性肠系膜静脉血栓形成触发因素的患者,应进行遗传性和获得性血栓形成倾向的血液筛查。
早期诊断需要进行急诊 CT 检查,静脉内注射造影剂增强门静脉期成像,并进行抗凝治疗,才能实现非手术成功的治疗过程。