D'Errico Stefano, Baldari Benedetta, Arcangeli Mauro, Santurro Alessandro, Frati Paola, Fineschi Vittorio
Department of Medicine, Surgery and Health, University of Trieste, Trieste.
Department of Anatomical, Histological, Forensic and Orthopaedic Sciences, Sapienza University of Rome, Rome.
Medicine (Baltimore). 2020 Oct 23;99(43):e22814. doi: 10.1097/MD.0000000000022814.
Although the cancer incidence continues to rise, cancer mortality has declined over the past decade, in large part due to more efficacious chemotherapeutic regimens thus, the ability to use first-line chemotherapeutic agents in the treatment of patients with cancer is crucial. Antineoplastic agents can potentially cause toxic and/or hypersensitivity reactions, that can have serious consequences. Anaphylaxis is a big pitfall in oncological patients; the most important aspect in diagnosing anaphylaxis is to precisely identify the offending agent to prevent future events. Paclitaxel (Taxol) is widely used as antitumor medication in the ovarian, breast, non-small-cell lung, and other cancers. Paclitaxel hypersensitivity reactions are frequently described in the literature, but fatalities are rarely reported. Due to the low solubility of paclitaxel, the compound requires dissolution in Cremophor EL, a derivative of castor oil.
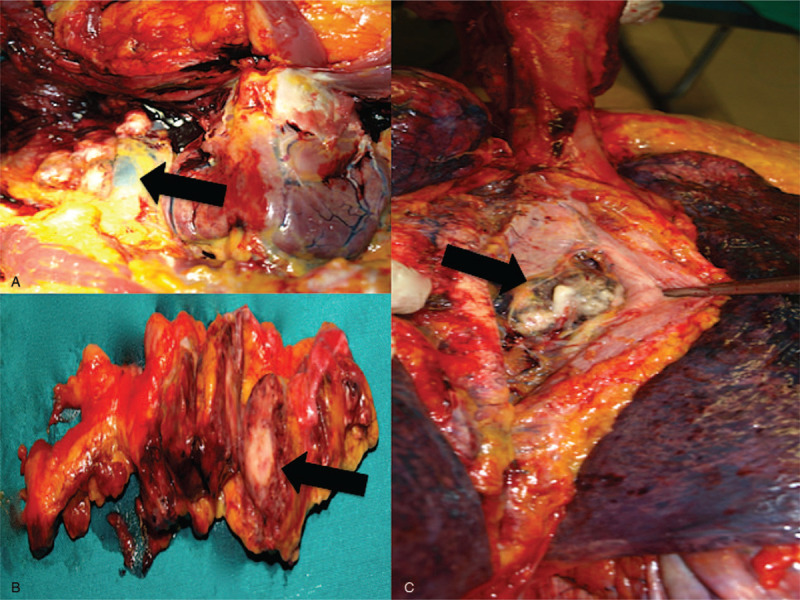
A 79-year-old man was affected by high-grade non-papillary urothelial carcinoma and underwent a radical cystectomy and prostatectomy with locoregional lymphadenectomy.
Eight months later, relapse was detected, and penis amputation and left nephrostomy were performed. Multiple metastases to lymph nodes were detected.
Palliative chemotherapy was started with Paclitaxel (110 mg) infused at a rate of 50 mL/h. Despite premedication with cetirizine dihydrochloride, dexamethasone, ondansetron, ranitidine, 20 min after Paclitaxel infusion starts, the patient developed general distress, followed by cardiac arrest.
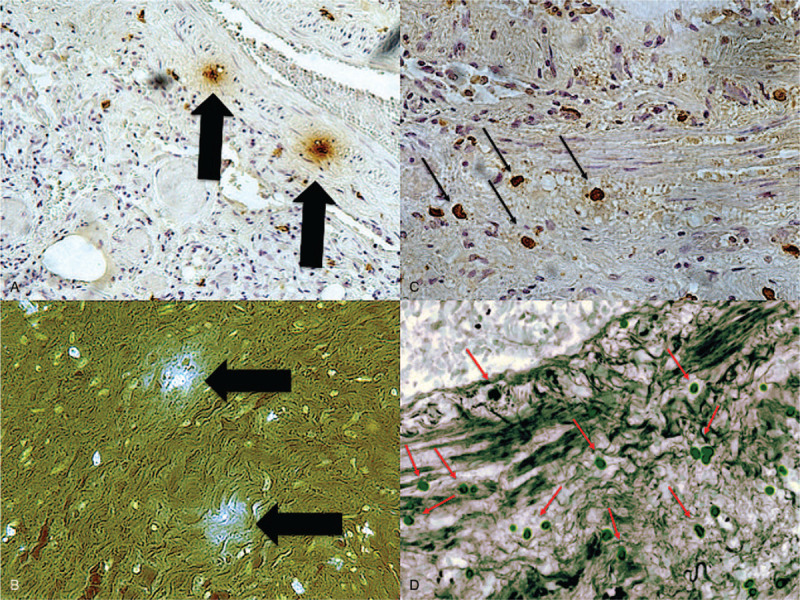
The mechanism of fatal paclitaxel-associated hypersensitivity reaction is uncertain and its solvent vehicle Cremophor EL may be involved. Several mechanisms have been postulated: an IgE-mediated mast cell degranulation induced by paclitaxel or Cremophor EL, a non-IgE-mediated idiosyncratic mast cell degranulation by paclitaxel or by Cremophor EL, and complement activation. Severe hypersensitivity reactions with fatal outcome are considered rare.
The unpredictability and often dramatic reactions of Taxol cause substantial anxiety for doctors and caretakers. They also represent a significant logistic and financial burden on hospitals. Despite premedication, skin testing, and desensitization protocols administration of taxane-based, chemotherapy cannot be considered safe and severe to fatal hypersensitivity reactions cannot be prevented.
尽管癌症发病率持续上升,但在过去十年中癌症死亡率有所下降,这在很大程度上归因于更有效的化疗方案。因此,使用一线化疗药物治疗癌症患者的能力至关重要。抗肿瘤药物可能会引起毒性和/或过敏反应,这些反应可能会产生严重后果。过敏反应是肿瘤患者的一个重大隐患;诊断过敏反应最重要的方面是准确识别引发反应的药物,以防止未来发生此类事件。紫杉醇(泰素)被广泛用作治疗卵巢癌、乳腺癌、非小细胞肺癌和其他癌症的抗肿瘤药物。紫杉醇过敏反应在文献中经常被描述,但死亡病例很少报道。由于紫杉醇的溶解度低,该化合物需要溶解在蓖麻油衍生物聚氧乙烯蓖麻油中。
一名79岁男性患有高级别非乳头状尿路上皮癌,接受了根治性膀胱切除术、前列腺切除术及局部区域淋巴结清扫术。
八个月后,检测到复发,进行了阴茎截肢术和左肾造瘘术。检测到多处淋巴结转移。
开始使用紫杉醇(110毫克)进行姑息化疗,以50毫升/小时的速度输注。尽管在使用紫杉醇前预先使用了盐酸西替利嗪、地塞米松、昂丹司琼、雷尼替丁,但在紫杉醇输注开始20分钟后,患者出现全身不适,随后心脏骤停。
与紫杉醇相关的致命过敏反应机制尚不确定,其溶剂聚氧乙烯蓖麻油可能与之有关。已提出几种机制:紫杉醇或聚氧乙烯蓖麻油诱导的IgE介导的肥大细胞脱颗粒、紫杉醇或聚氧乙烯蓖麻油引起的非IgE介导的特异质肥大细胞脱颗粒以及补体激活。严重过敏反应导致死亡的情况被认为很少见。
紫杉醇不可预测且常常引发剧烈反应,给医生和护理人员带来了极大的焦虑。它们也给医院带来了巨大的后勤和经济负担。尽管进行了预处理、皮肤试验和脱敏方案,但基于紫杉烷的化疗仍不能被认为是安全的,严重至致命的过敏反应无法预防。