1Department of Ophthalmology, Virginia Commonwealth University, Richmond, Virginia.
2Department of Ophthalmology, Hunter Holmes McGuire VA Medical Center, Richmond, Virginia.
Am J Trop Med Hyg. 2020 Dec;103(6):2400-2411. doi: 10.4269/ajtmh.20-1015. Epub 2020 Oct 26.
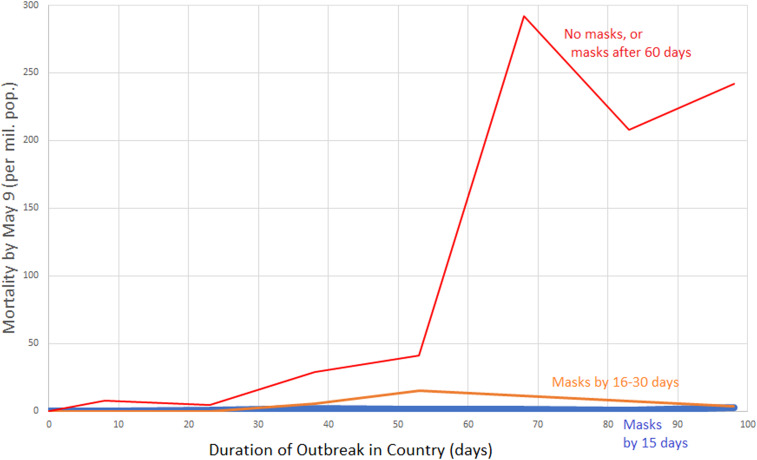
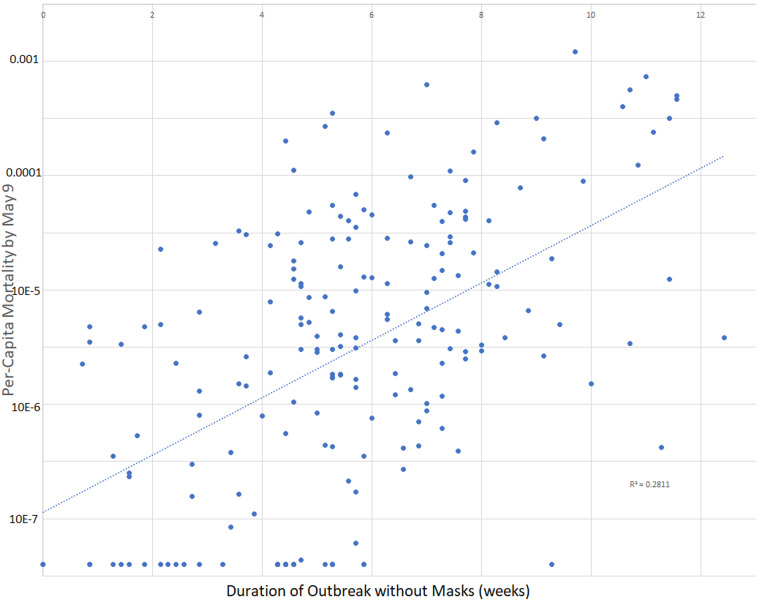
We studied sources of variation between countries in per-capita mortality from COVID-19 (caused by the SARS-CoV-2 virus). Potential predictors of per-capita coronavirus-related mortality in 200 countries by May 9, 2020 were examined, including age, gender, obesity prevalence, temperature, urbanization, smoking, duration of the outbreak, lockdowns, viral testing, contact-tracing policies, and public mask-wearing norms and policies. Multivariable linear regression analysis was performed. In univariate analysis, the prevalence of smoking, per-capita gross domestic product, urbanization, and colder average country temperature were positively associated with coronavirus-related mortality. In a multivariable analysis of 196 countries, the duration of the outbreak in the country, and the proportion of the population aged 60 years or older were positively associated with per-capita mortality, whereas duration of mask-wearing by the public was negatively associated with mortality (all < 0.001). Obesity and less stringent international travel restrictions were independently associated with mortality in a model which controlled for testing policy. Viral testing policies and levels were not associated with mortality. Internal lockdown was associated with a nonsignificant 2.4% reduction in mortality each week ( = 0.83). The association of contact-tracing policy with mortality was not statistically significant ( = 0.06). In countries with cultural norms or government policies supporting public mask-wearing, per-capita coronavirus mortality increased on average by just 16.2% each week, as compared with 61.9% each week in remaining countries. Societal norms and government policies supporting the wearing of masks by the public, as well as international travel controls, are independently associated with lower per-capita mortality from COVID-19.
我们研究了各国 COVID-19(由 SARS-CoV-2 病毒引起)人均死亡率差异的来源。我们研究了 200 个国家截至 2020 年 5 月 9 日的与冠状病毒相关的人均死亡率的潜在预测因子,包括年龄、性别、肥胖症患病率、温度、城市化、吸烟、疫情持续时间、封锁、病毒检测、接触者追踪政策以及公众戴口罩的规范和政策。我们进行了多变量线性回归分析。在单变量分析中,吸烟流行率、人均国内生产总值、城市化和较冷的国家平均温度与冠状病毒相关死亡率呈正相关。在对 196 个国家的多变量分析中,国内疫情持续时间以及 60 岁或以上人口比例与人均死亡率呈正相关,而公众戴口罩的持续时间与死亡率呈负相关(均<0.001)。在控制了检测政策的模型中,肥胖症和更宽松的国际旅行限制与死亡率独立相关。病毒检测政策和水平与死亡率无关。内部封锁与死亡率每周降低 2.4%(β=0.83)无显著关联。接触者追踪政策与死亡率的关联没有统计学意义(β=0.06)。在具有支持公众戴口罩的文化规范或政府政策的国家中,冠状病毒人均死亡率每周平均增加 16.2%,而在其余国家中,冠状病毒人均死亡率每周增加 61.9%。支持公众戴口罩的社会规范和政府政策以及国际旅行控制措施与 COVID-19 的人均死亡率降低独立相关。