Department of Intensive Care, Erasme Hospital, Université Libre de Bruxelles (ULB), Route de Lennik, 808, 1070, Brussels, Belgium.
Department of Medical Biotechnologies, Anesthesia and Intensive Care Unit, University of Siena, Via Bracci 1, 53100, Siena, Italy.
Crit Care. 2020 Oct 30;24(1):629. doi: 10.1186/s13054-020-03353-z.
Neurologic injury is one of the most frequent causes of death in patients undergoing extracorporeal membrane oxygenation (ECMO). As neurological examination is often unreliable in sedated patients, additional neuromonitoring is needed. However, the value of electroencephalogram (EEG) in adult ECMO patients has not been well assessed. Therefore, the aim of this study was to assess the occurrence of electroencephalographic abnormalities in patients treated with extracorporeal membrane oxygenation (ECMO) and their association with 3-month neurologic outcome.
Retrospective analysis of all patients undergoing venous-venous (V-V) or venous-arterial (V-A) ECMO with a concomitant EEG recording (April 2009-December 2018), either recorded intermittently or continuously. EEG background was classified into four categories: mild/moderate encephalopathy (i.e., mostly defined by the presence of reactivity), severe encephalopathy (mostly defined by the absence of reactivity), burst-suppression (BS) and suppressed background. Epileptiform activity (i.e., ictal EEG pattern, sporadic epileptiform discharges or periodic discharges) and asymmetry were also reported. EEG findings were analyzed according to unfavorable neurological outcome (UO, defined as Glasgow Outcome Scale < 4) at 3 months after discharge.
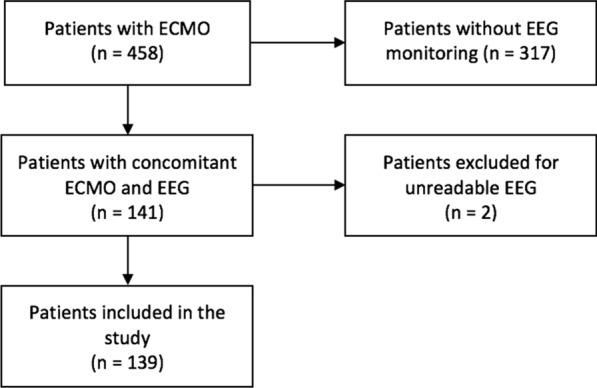
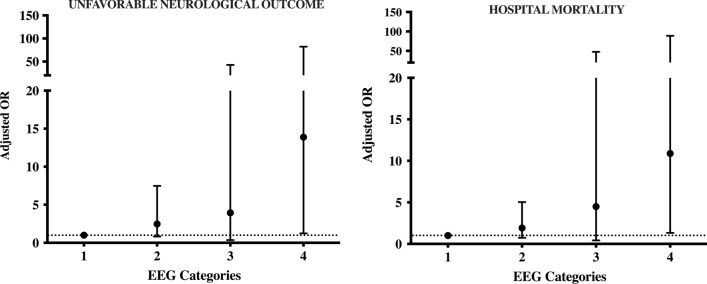
A total of 139 patients (54 [41-62] years; 60 (43%) male gender) out of 596 met the inclusion criteria and were analyzed. Veno-arterial (V-A) ECMO was used in 98 (71%); UO occurred in 99 (71%) patients. Continuous EEG was performed in 113 (81%) patients. The analysis of EEG background showed that 29 (21%) patients had severe encephalopathy, 4 (3%) had BS and 19 (14%) a suppressed background. In addition, 11 (8%) of patients had seizures or status epilepticus, 10 (7%) had generalized periodic discharges or lateralized periodic discharges, and 27 (19%) had asymmetry on EEG. In the multivariate analysis, the occurrence of ischemic stroke or intracranial hemorrhage (OR 4.57 [1.25-16.74]; p = 0.02) and a suppressed background (OR 10.08 [1.24-82.20]; p = 0.03) were independently associated with UO. After an adjustment for covariates, an increasing probability for UO was observed with more severe EEG background categories.
In adult patients treated with ECMO, EEG can identify patients with a high likelihood of poor outcome. In particular, suppressed background was independently associated with unfavorable neurological outcome.
神经系统损伤是体外膜肺氧合(ECMO)患者死亡的最常见原因之一。由于镇静患者的神经系统检查往往不可靠,因此需要额外的神经监测。然而,脑电图(EEG)在成人 ECMO 患者中的价值尚未得到很好的评估。因此,本研究旨在评估接受体外膜肺氧合(ECMO)治疗的患者中脑电图异常的发生情况及其与 3 个月神经预后的关系。
对 2009 年 4 月至 2018 年 12 月期间接受静脉-静脉(V-V)或静脉-动脉(V-A)ECMO 治疗并同时进行脑电图记录的所有患者进行回顾性分析,记录方式为间歇性或连续记录。脑电图背景分为四类:轻度/中度脑病(即主要表现为反应性)、重度脑病(主要表现为无反应性)、爆发抑制(BS)和抑制性背景。还报告了癫痫样活动(即发作性脑电图模式、散发性癫痫样放电或周期性放电)和不对称性。根据出院后 3 个月的不良神经结局(定义为格拉斯哥结局量表评分<4)分析脑电图结果。
共纳入 596 例患者中的 139 例(54[41-62]岁;60[43%]为男性),并对其进行了分析。98 例(71%)患者接受了静脉-动脉(V-A)ECMO;99 例(71%)患者发生不良神经结局。113 例(81%)患者进行了连续脑电图检查。脑电图背景分析显示,29 例(21%)患者有重度脑病,4 例(3%)有 BS,19 例(14%)有抑制性背景。此外,11 例(8%)患者有癫痫发作或癫痫持续状态,10 例(7%)患者有全面性周期性放电或局灶性周期性放电,27 例(19%)患者脑电图有不对称性。多变量分析显示,缺血性卒中和颅内出血(OR 4.57[1.25-16.74];p=0.02)和抑制性背景(OR 10.08[1.24-82.20];p=0.03)与不良神经结局独立相关。在调整协变量后,随着脑电图背景严重程度的增加,不良神经结局的可能性逐渐增加。
在接受 ECMO 治疗的成人患者中,脑电图可识别出预后不良的高风险患者。特别是,抑制性背景与不良神经结局独立相关。