Rodrigues Adriana Teixeira, Rodrigues Julia Teixeira, Rodrigues Carolina Teixeira, Volpe Caroline Maria de Oliveira, Rocha-Silva Fabiana, Nogueira-Machado Jose Augusto, Alberti Luiz Ronaldo
Department of Pediatrics, School of Medicine, Federal University of Minas Gerais, Belo Horizonte 30130-100, Minas Gerais, Brazil.
Department of Pharmacy, Federal University of Minas Gerais, Belo Horizonte 31270-901, Minas Gerais, Brazil.
World J Crit Care Med. 2020 Oct 18;9(4):63-73. doi: 10.5492/wjccm.v9.i4.63.
High mobility group box 1 (HMGB1) has been studied as a molecule associated with severe outcomes in sepsis and thrombomodulin (TM) seems to decrease HMGB1 activity.
To investigate the role of the thrombomodulin/high mobility group box 1 (T/H) ratio in patients with sepsis and their association with their clinic, testing the hypothesis that higher ratios are associated with better outcomes.
Twenty patients diagnosed with sepsis or septic shock, according to the 2016 criteria sepsis and septic shock (Sepsis-3), were studied. Patients were followed until they left the intensive care unit or until they achieved 28 d of hospitalization (D28). The following clinical outcomes were observed: Sequential Organ Failure Assessment (SOFA) score; Need for mechanical pulmonary ventilation; Presence of septic shock; Occurrence of sepsis-induced coagulopathy; Need for renal replacement therapy (RRT); and Death.
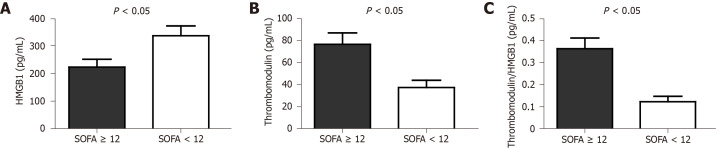
The results showed that patients with SOFA scores greater than or equal to 12 points had higher serum levels of TM: 76.41 ± 29.21 pg/mL 37.41 ± 22.55 pg/mL among those whose SOFA scores were less than 12 points, = 0.003. The T/H ratio was also higher in patients whose SOFA scores were greater than or equal to 12 points, = 0.001. The T/H ratio was, on average, three times higher in patients in need of RRT (0.38 ± 0.14 0.11 ± 0.09), < 0.001.
Higher serum levels of TM and, therefore, higher T/H ratio in the first 24 h after the diagnosis of sepsis were associated with more severe disease and the need for renal replacement therapy, while those with better clinical outcomes and those who were discharged before D28 showed a tendency for lower T/H ratio values.
高迁移率族蛋白B1(HMGB1)作为一种与脓毒症严重预后相关的分子已被研究,而血栓调节蛋白(TM)似乎可降低HMGB1活性。
探讨血栓调节蛋白/高迁移率族蛋白B1(T/H)比值在脓毒症患者中的作用及其与临床情况的关联,检验更高比值与更好预后相关的假设。
根据2016年脓毒症和脓毒性休克标准(Sepsis - 3),对20例诊断为脓毒症或脓毒性休克的患者进行研究。对患者进行随访,直至其离开重症监护病房或住院达到28天(D28)。观察以下临床结局:序贯器官衰竭评估(SOFA)评分;机械通气需求;脓毒性休克的存在;脓毒症诱导的凝血病的发生;肾脏替代治疗(RRT)需求;以及死亡。
结果显示,SOFA评分大于或等于12分的患者血清TM水平更高:SOFA评分小于12分的患者中TM水平为37.41±22.55 pg/mL,而SOFA评分大于或等于12分的患者中TM水平为76.41±29.21 pg/mL,P = 0.003。SOFA评分大于或等于12分的患者T/H比值也更高,P = 0.001。需要RRT的患者T/H比值平均高出三倍(0.38±0.14对0.11±0.09),P < 0.001。
脓毒症诊断后最初24小时内血清TM水平较高,因此T/H比值较高,与更严重的疾病和肾脏替代治疗需求相关,而临床结局较好且在D28之前出院的患者T/H比值有降低趋势。