Pennell Christopher, Meckmongkol Teerin, Arthur L Grier, Ciullo Sean, Prasad Rajeev, Lindholm Erika, Grewal Harsh
St. Christopher's Hospital for Children, Department of Pediatric General, Thoracic, and Minimally Invasive Pediatric Surgery, Philadelphia, Pa.
Department of Surgery, Drexel University College of Medicine, Philadelphia, Pa.
Pediatr Qual Saf. 2020 Oct 26;5(6):e357. doi: 10.1097/pq9.0000000000000357. eCollection 2020 Nov-Dec.
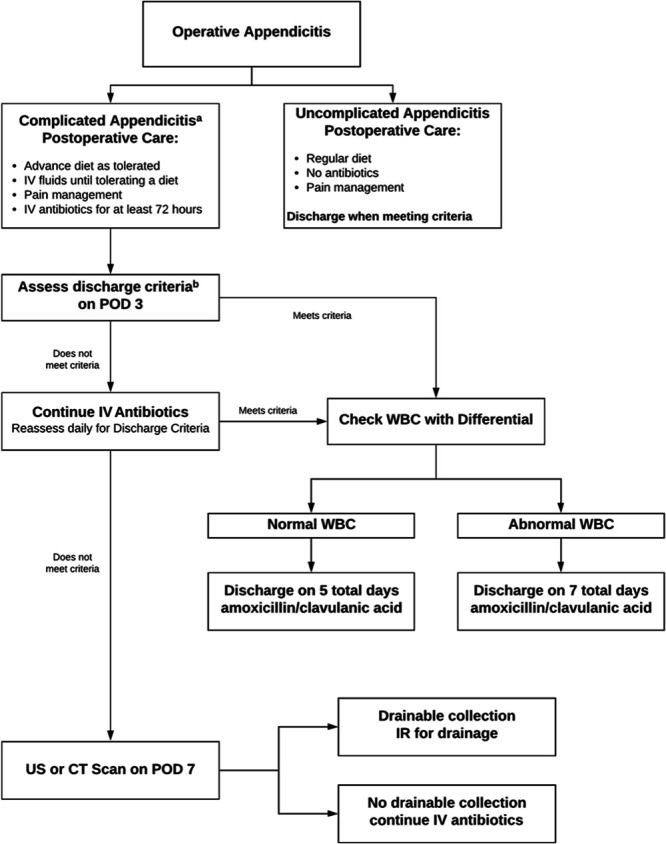
Appendicitis is the most common condition requiring emergency surgery in children. We implemented a standardized protocol (SP) for treating children with appendicitis to provide more uniform care and reduce resource utilization.
All patients younger than 21 years were managed with the SP beginning in January 2017. We compared data from 22 months before and after implementation. The primary outcomes included the length of stay (LOS), antibiotic days, discharge on intravenous antibiotics, utilization of peripherally inserted central catheters lines, and postoperative imaging. Secondary outcomes were protocol adherence and the rates adverse events, including postoperative abscess, return to emergency department or operating room, surgical site infection, and readmission.
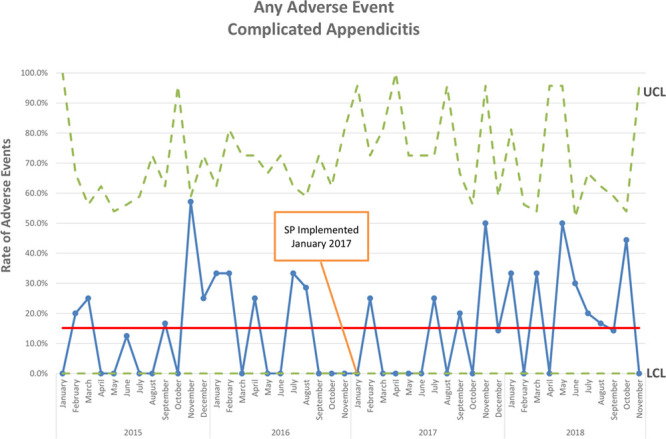
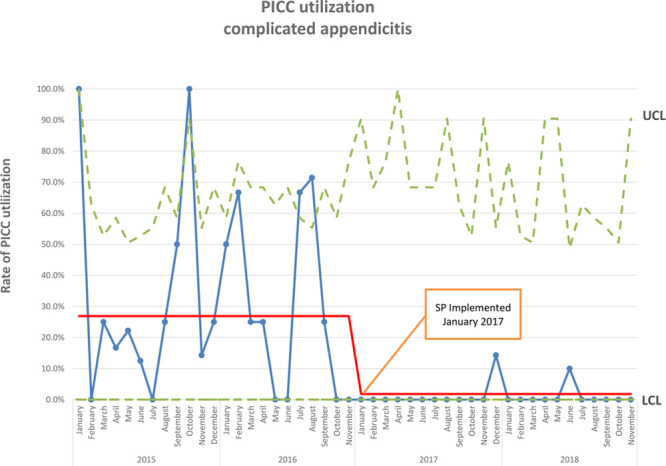
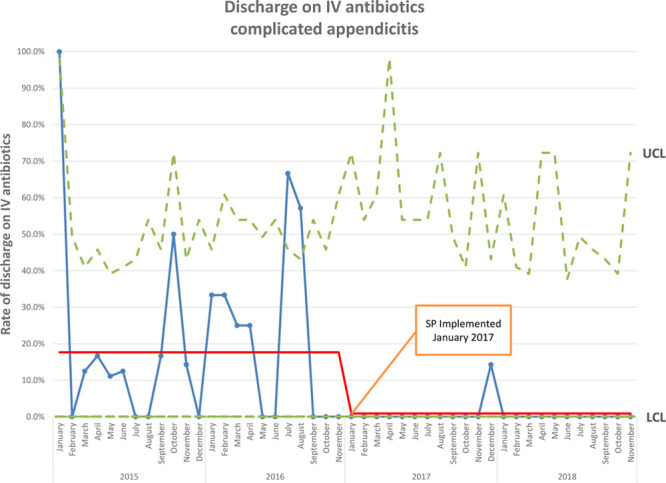
Protocol adherence was 92.3%. For uncomplicated cases (n = 412), LOS ( = 0.010) and postoperative antibiotic days ( < 0.001) were significantly reduced. There was no difference in the rates of any adverse event (6.7% versus 2.7%; = 0.058), postoperative abscess (0.4% versus 0.0%; = 0.544), return to emergency department (6.3% versus 2.7%; = 0.084), readmission (1.8% versus 0.5%; = 0.245), or postoperative ultrasound (0.4% versus 0.5%; = 0.705) and computed tomography (0.0% versus 0.5%; = 0.456). For complicated cases (n = 229), the post-SP cohort had a shorter LOS ( = 0.015), fewer peripherally inserted central catheters lines (26.9% versus 2.7%; < 0.001), fewer postoperative ultrasounds (8.4% versus 1.8%; = 0.027), and fewer discharges on intravenous antibiotics (17.6% versus 0.9%; < 0.001). There were no differences in adverse events before and after the SP (16.0% versus 18.3%; = 0.633).
Implementing an SP for appendicitis in children reduced resource utilization, and by inference healthcare costs, for both uncomplicated and complicated cases without adversely affecting clinical outcomes.
阑尾炎是儿童最常见的需要急诊手术的疾病。我们实施了一项治疗儿童阑尾炎的标准化方案(SP),以提供更统一的护理并减少资源利用。
自2017年1月起,所有21岁以下的患者均采用SP进行管理。我们比较了实施前后22个月的数据。主要结局包括住院时间(LOS)、抗生素使用天数、静脉使用抗生素出院情况、外周静脉穿刺中心静脉导管的使用情况以及术后影像学检查。次要结局是方案依从性和不良事件发生率,包括术后脓肿、返回急诊科或手术室、手术部位感染和再次入院。
方案依从率为92.3%。对于非复杂病例(n = 412),住院时间( = 0.010)和术后抗生素使用天数( < 0.001)显著缩短。任何不良事件发生率(6.7%对2.7%; = 0.058)、术后脓肿发生率(0.4%对0.0%; = 0.544)、返回急诊科发生率(6.3%对2.7%; = 0.084)、再次入院发生率(1.8%对0.5%; = 0.245)、术后超声检查发生率(0.4%对0.5%; = 0.705)和计算机断层扫描发生率(0.0%对0.5%; = 0.456)均无差异。对于复杂病例(n = 229),SP实施后队列的住院时间更短( = 0.015),外周静脉穿刺中心静脉导管使用更少(26.9%对2.7%; < 0.001),术后超声检查更少(8.4%对1.8%; = 0.027),静脉使用抗生素出院更少(从17.6%降至0.9%; < 0.001)。SP实施前后不良事件发生率无差异(16.0%对18.3%; = 0.633)。
在儿童阑尾炎治疗中实施SP可降低非复杂和复杂病例的资源利用,进而推断可降低医疗成本,且不会对临床结局产生不利影响。