Global Health, Bill & Melinda Gates Foundation, Seattle, WA.
HIV Programmes & Advocacy, International AIDS Society, Cape Town, South Africa.
J Acquir Immune Defic Syndr. 2021 Feb 1;86(2):147-152. doi: 10.1097/QAI.0000000000002549.
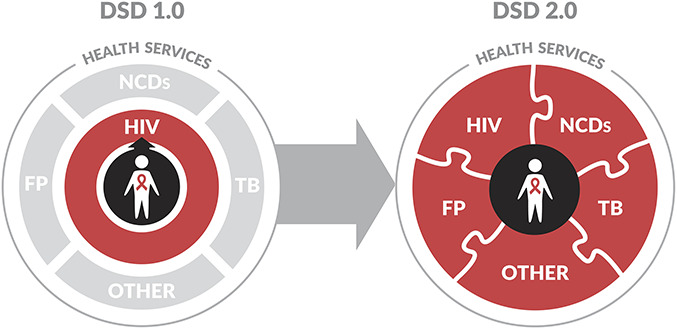
Simplifying antiretroviral therapy for clinically stable people living with HIV (PLHIV) is important but insufficient to meet their health care needs, including prevention and treatment of tuberculosis and noncommunicable diseases, routine primary care, and family planning. Integrating these services into differentiated service delivery (DSD) platforms is a promising avenue to achieve such coverage. We propose a transition from an HIV-focused "DSD 1.0" to a patient-centered "DSD 2.0" that is inclusive of additional chronic care services for PLHIV.
The lack of coordination between HIV programs and these critical services puts a burden on both PLHIV and health systems. For individual patients, fractionated services increase cost and time, diminish the actual and perceived quality of care, and increase the risk that they will disengage from health care altogether. The burden on the health system is one of inefficiency and suboptimal outcomes resulting from the parallel systems required to manage multiple vertical programs.
DSD 2.0 provides an opportunity for the HIV and Universal Health Coverage agendas-which can seem to be at odds-to achieve greater collective impact for patients and health systems by integrating strong vertical HIV, tuberculosis and family planning programs, and relatively weaker noncommunicable disease programs. Increasing coordination of care for PLHIV will increase the likelihood of achieving and sustaining UNAIDS' goals of retention on antiretroviral therapy and viral suppression. Eventually, this shift to DSD 2.0 for PLHIV could evolve to a more person-centered vision of chronic care services that would also serve the general population.
简化对临床稳定的 HIV 感染者(PLHIV)的抗逆转录病毒治疗很重要,但这还不足以满足他们的医疗保健需求,包括预防和治疗结核病和非传染性疾病、常规初级保健和计划生育。将这些服务纳入差异化服务提供(DSD)平台是实现这种覆盖的一个有前途的途径。我们建议从以 HIV 为重点的“DSD 1.0”向以患者为中心的“DSD 2.0”过渡,该模式将包括 PLHIV 额外的慢性护理服务。
HIV 项目与这些关键服务之间缺乏协调,给 PLHIV 和卫生系统带来了负担。对于个体患者来说,分散的服务增加了成本和时间,降低了实际和感知到的护理质量,并增加了他们完全脱离医疗保健的风险。对卫生系统的负担是由于需要管理多个垂直项目而导致效率低下和结果不佳的一个原因。
DSD 2.0 为 HIV 和全民健康覆盖议程提供了一个机会——这两个议程似乎存在冲突——通过整合强大的垂直 HIV、结核病和计划生育项目,以及相对较弱的非传染性疾病项目,为患者和卫生系统实现更大的集体影响。增加对 PLHIV 的护理协调将增加实现和维持艾滋病规划署关于抗逆转录病毒治疗和病毒抑制保留率的目标的可能性。最终,这种向 PLHIV 的 DSD 2.0 的转变可能会发展为更以患者为中心的慢性护理服务愿景,也将为一般人群服务。