Póvoa Antónia Afonso, Teixeira Elisabete, Bella-Cueto Maria Rosa, Melo Miguel, Oliveira Maria João, Sobrinho-Simões Manuel, Maciel Jorge, Soares Paula
Department of General Surgery, Centro Hospitalar de Vila Nova de Gaia/Espinho (CHVNG/E), 4434-502 Gaia, Portugal.
IPATIMUP-Instituto de Patologia e Imunologia Molecular, Universidade do Porto, 4200-135 Porto, Portugal.
Cancers (Basel). 2020 Oct 29;12(11):3186. doi: 10.3390/cancers12113186.
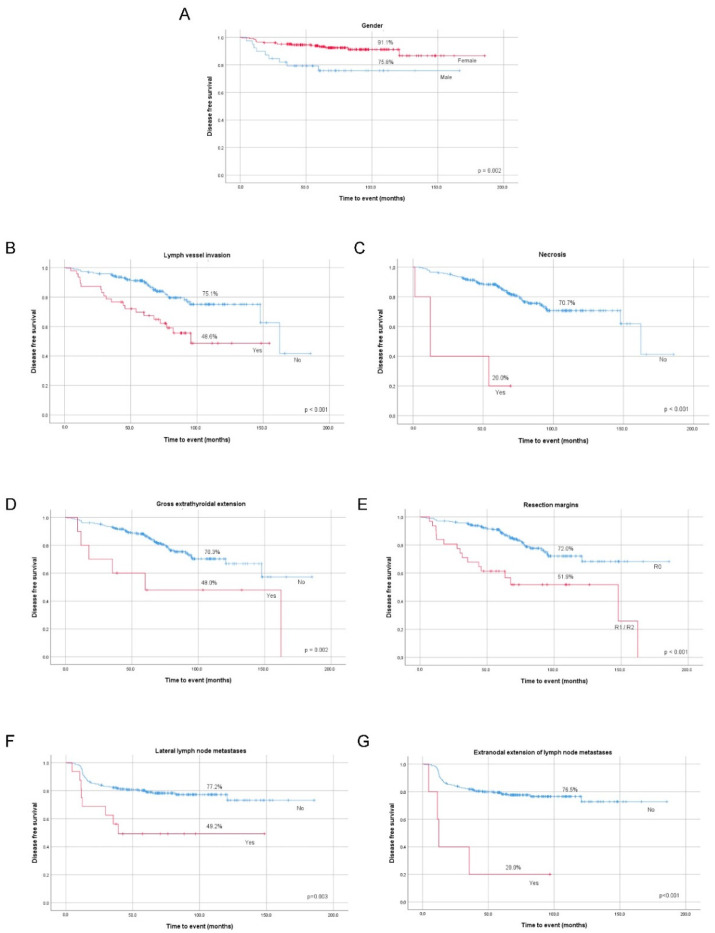
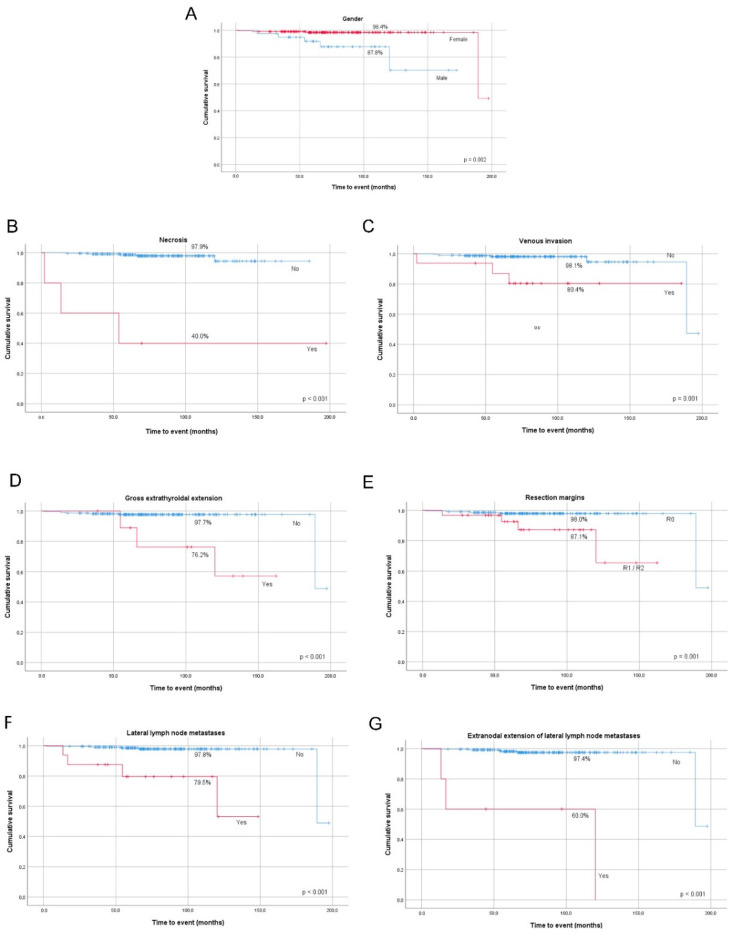
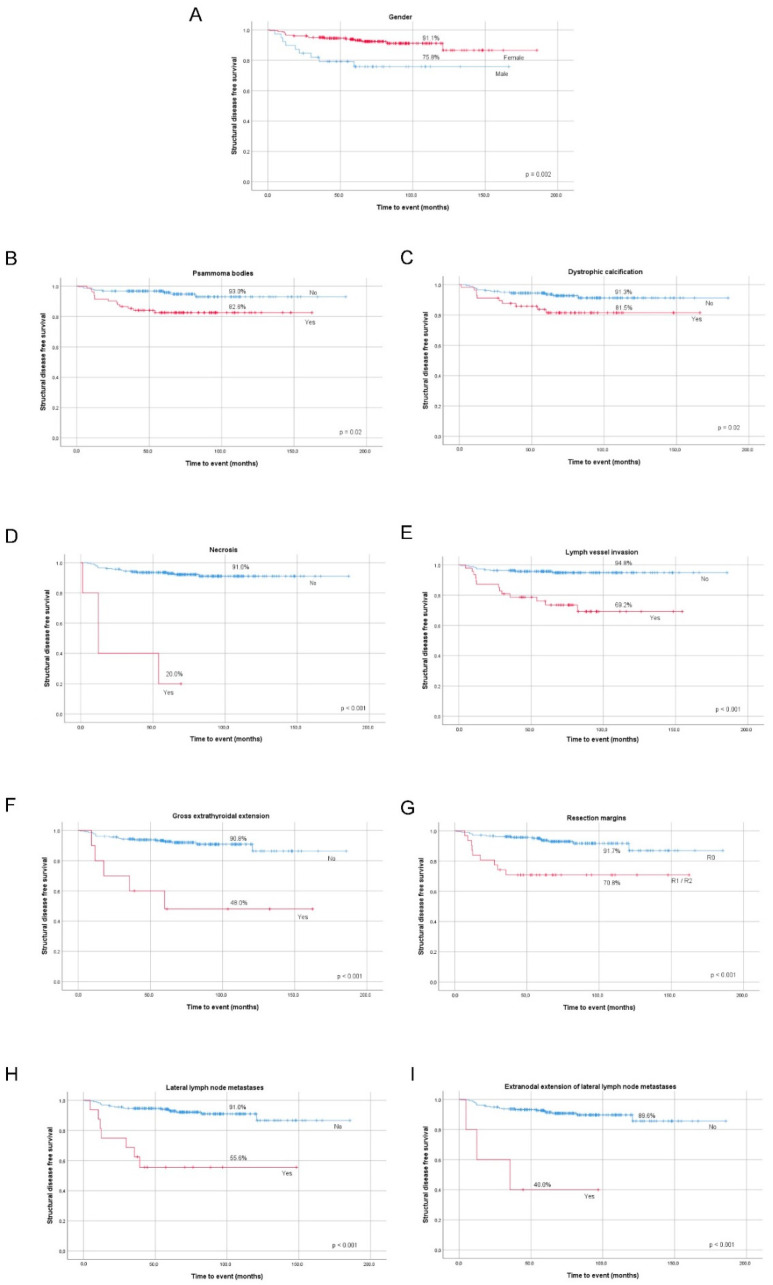
Papillary thyroid cancer (PTC) has an indolent nature and usually excellent prognosis. Some PTC clinicopathological features may contribute to the development of aggressive metastatic disease. In this work, we want to evaluate PTC clinicopathological features that are presurgical prognostic predictors of patients' outcomes and find which indicators are more adequate for tailoring surgical procedures and follow-up. We studied a series of 241 PTC patients submitted to surgery. All patients' files and histological tumor samples were reviewed. The 8th edition AJCC/UICC (American Joint Committee on Cancer/Union for International Cancer) Controlstaging system and the 2015 American Thyroid Association risk stratification system were used. Total thyroidectomy was performed in 228 patients, lymphadenectomy in 28 patients. Gross extrathyroidal extension (ETE) was present in 10 patients and 31 tumor resection margins were incomplete. Cervical lymph node metastases (LNMs) were present in 34 patients and distant metastases at diagnosis in four patients. In multivariate analysis, male gender (OR = 15.4, = 0.015), venous invasion (OR = 16.7, = 0.022), and lateral compartment LNM (OR = 26.7, = 0.004) were predictors of mortality; psammoma bodies (PBs) (OR = 4.5, = 0.008), lymph vessel invasion (OR = 6.9, < 0.001), and gross ETE (OR = 16.1, = 0.001) were predictors of structural disease status; male gender (OR = 2.9, = 0.011), lymph vessel invasion (OR = 2.8, = 0.006), and incomplete resection margins (OR = 4.6, < 0.001) were predictors of recurrent/persistent disease. Our study supports that the factors helping to tailor patient's surgery are male gender, presence of PBs, gross ETE, and lateral compartment LNM. Together with pathological factors, lymph vessel invasion, venous invasion, necrosis, and incomplete surgical resection, should be taken into consideration regarding treatment and follow-up of patients.
甲状腺乳头状癌(PTC)具有惰性本质,通常预后良好。一些PTC的临床病理特征可能促使侵袭性转移性疾病的发生。在本研究中,我们旨在评估PTC的临床病理特征,这些特征是患者预后的术前预测指标,并找出哪些指标更适合用于指导手术操作和随访。我们研究了241例行手术治疗的PTC患者。回顾了所有患者的病历和肿瘤组织样本。采用美国癌症联合委员会/国际癌症联盟(AJCC/UICC)第8版分期系统和2015年美国甲状腺协会风险分层系统。228例患者行甲状腺全切除术,28例患者行淋巴结清扫术。10例患者存在肉眼可见的甲状腺外侵犯(ETE),31例患者肿瘤切除切缘不完整。34例患者存在颈部淋巴结转移(LNM),4例患者诊断时存在远处转移。多因素分析显示,男性(OR = 15.4,P = 0.015)、血管侵犯(OR = 16.7,P = 0.022)和侧方区LNM(OR = 26.7,P = 0.004)是死亡的预测因素;砂粒体(PBs)(OR = 4.5,P = 0.008)、淋巴管侵犯(OR = 6.9,P < 0.001)和肉眼可见的ETE(OR = 16.1,P = 0.001)是结构疾病状态的预测因素;男性(OR = 2.9,P = 0.011)、淋巴管侵犯(OR = 2.8,P = 0.006)和切缘不完整(OR = 4.6,P < 0.001)是复发/持续性疾病的预测因素。我们的研究支持,有助于指导患者手术的因素包括男性、PBs的存在、肉眼可见的ETE和侧方区LNM。在考虑患者的治疗和随访时,应将淋巴管侵犯、血管侵犯、坏死和手术切除不完整等病理因素一并考虑在内。