Department of Neurosurgery, Technical University Munich, Medical Faculty, School of Medicine, Klinikum rechts der Isar, Ismaninger Str. 22, 81675, Munich, Germany.
Department of Neuropathology, Technical University Munich, School of Medicine, Klinikum rechts der Isar, Institute of Pathology, Munich, Germany.
BMC Cancer. 2020 Nov 3;20(1):1060. doi: 10.1186/s12885-020-07570-1.
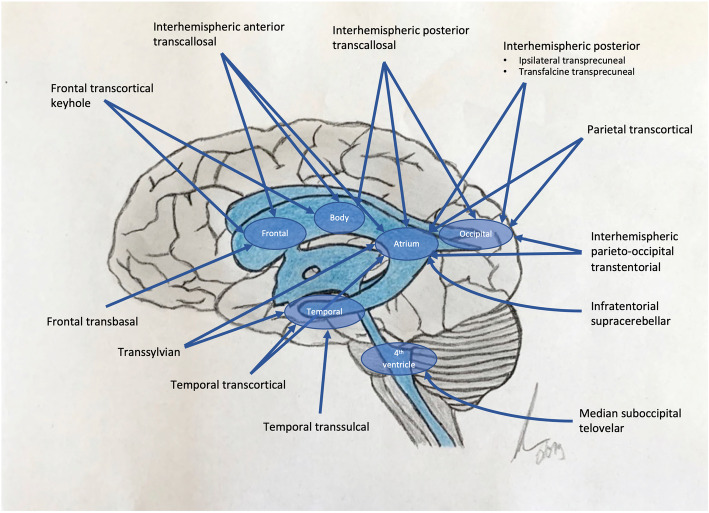
Intraventricular neuroepithelial tumors (IVT) are rare lesions and comprise different pathological entities such as ependymomas, subependymomas and central neurocytomas. The treatment of choice is neurosurgical resection, which can be challenging due to their intraventricular location. Different surgical approaches to the ventricles are described. Here we report a large series of IVTs, its postoperative outcome at a single tertiary center and discuss suitable surgical approaches.
We performed a retrospective chart review at a single tertiary neurosurgical center between 03/2009-05/2019. We included patients that underwent resection of an IVT emphasizing on surgical approach, extent of resection, clinical outcome and postoperative complications.
Forty five IVTs were resected from 03/2009 to 05/2019, 13 ependymomas, 21 subependymomas, 10 central neurocytomas and one glioependymal cyst. Median age was 52,5 years with 55.6% (25) male and 44.4% (20) female patients. Gross total resection was achieved in 93.3% (42/45). 84.6% (11/13) of ependymomas, 100% (12/21) of subependymomas, 90% (9/10) of central neurocytomas and one glioependymal cyst were completely removed. Postoperative rate of new neurological deficits was 26.6% (12/45). Postoperative new permanent cranial nerve deficits occurred in one case with 4th ventricle subependymoma and one in 4th ventricle ependymoma. Postoperative KPSS was 90% (IR 80-100). 31.1% of the patients improved in KPSS, 48.9% remained unchanged and 20% declined. Postoperative adverse events rate was 20.0%. Surgery-related mortality was 2.2%. The rate of shunt/cisternostomy-dependent hydrocephalus was 13.3% (6/45). 15.4% of resected ependymomas underwent adjuvant radiotherapy. Mean follow-up was 26,9 (±30.1) months.
Our surgical findings emphasize satisfactory complete resection throughout all entities. Surgical treatment can remain feasible, if institutional experience is given. Satisfying long-term survival and cure is possible by complete removal. Gross total resection should always be performed under function-remaining aspects due to mostly benign or slow growing nature of IVTs. Further data is needed to evaluate standard of care and alternative therapy options in rare cases of tumor recurrence or in case of patient collective not suitable for operative resection.
脑室内神经上皮肿瘤(IVT)是一种罕见的病变,包括不同的病理实体,如室管膜瘤、室管膜下瘤和中枢神经细胞瘤。首选的治疗方法是神经外科切除术,但由于其位于脑室内,手术具有挑战性。有不同的手术方法用于治疗脑室病变。在这里,我们报告了一系列在单一三级中心治疗的 IVT 病例,探讨了其术后结果,并讨论了合适的手术方法。
我们对 2009 年 3 月至 2019 年 5 月期间在一家三级神经外科中心进行了回顾性病历审查。我们纳入了接受 IVT 切除术的患者,重点关注手术方法、切除程度、临床结果和术后并发症。
从 2009 年 3 月至 2019 年 5 月,共切除了 45 例 IVT,包括 13 例室管膜瘤、21 例室管膜下瘤、10 例中枢神经细胞瘤和 1 例胶样囊肿。中位年龄为 52.5 岁,55.6%(25 例)为男性,44.4%(20 例)为女性。93.3%(42/45)的患者达到了大体全切除。84.6%(11/13)的室管膜瘤、100%(12/21)的室管膜下瘤、90%(9/10)的中枢神经细胞瘤和 1 例胶样囊肿被完全切除。术后新发神经功能缺损的发生率为 26.6%(12/45)。术后新发第四脑室室管膜瘤和第四脑室室管膜瘤患者出现颅神经永久损伤。术后 KPSS 为 90%(IR 80-100)。31.1%的患者 KPSS 评分改善,48.9%的患者保持不变,20%的患者评分下降。术后不良事件发生率为 20.0%。手术相关死亡率为 2.2%。需要分流/脑池造瘘术的脑积水发生率为 13.3%(6/45)。15.4%的切除室管膜瘤患者接受了辅助放疗。中位随访时间为 26.9(±30.1)个月。
我们的手术结果强调了在所有实体中实现满意的完全切除。如果机构经验丰富,手术治疗仍然可行。通过完全切除可以获得满意的长期生存和治愈。由于 IVT 多为良性或生长缓慢,在保留功能的前提下,应尽可能进行大体全切除。需要进一步的数据来评估在罕见的肿瘤复发或不适合手术切除的患者群体中,治疗的标准和替代治疗选择。