Maisat Wiriya, Siriratwarangkul Sasiya, Charoensri Apiporn, Wongkornrat Wanchai, Lapmahapaisan Saowaphak
Department of Anesthesiology, Department of surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
Division of Cardiothoracic surgery, Department of surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
J Thorac Dis. 2020 Sep;12(9):4796-4804. doi: 10.21037/jtd-20-742.
Delayed extubation after cardiac surgery is associated with high morbidity and mortality, increased intensive care unit length of stay, and healthcare cost. Acute type A aortic dissection (ATAAD) generally results in prolonged mechanical ventilation due to the complexity of surgical management and some postoperative complications. This study aimed to elucidate the perioperative risk factors for delayed extubation in patients undergoing ATAAD surgery.
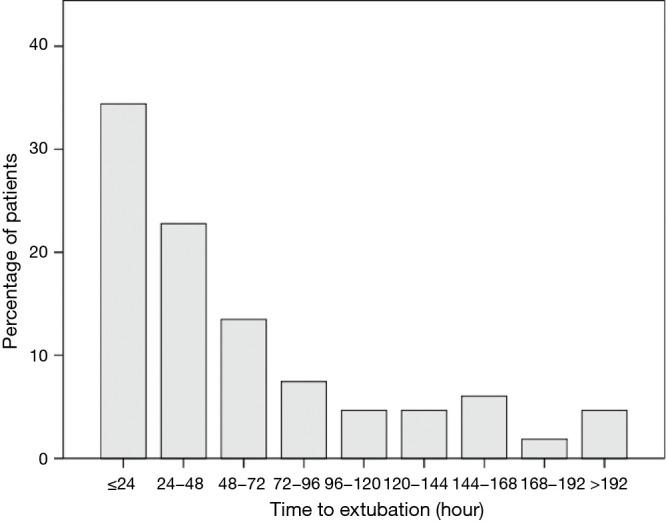
A retrospective cohort study including 239 patients who were diagnosed with ATAAD and underwent emergency surgery from October 2004 to January 2018 was performed. The potential perioperative risk factors for delayed extubation were collected. This study defined delayed extubation as the time to commence extubation being greater than 48 hours. The clinical data were analyzed with univariate and multivariate analyses to identify risk factors for delayed extubation following ATAAD surgery.
The incidence of delayed extubation was 48.5% (n=116). Multiple logistic regression analysis showed perioperative risk factors for delayed extubation included preoperative cardiac tamponade [odds ratio (OR) 3.94, 95% confidence interval (CI) 1.39-11.17, P=0.010], central arterial cannulation (ascending aorta and proximal aortic arch) for cardiopulmonary bypass (CPB) (OR 4.04, 95% CI: 1.03-15.91, P=0.046), postoperative stroke (OR 10.58, 95% CI: 2.65-42.25, P=0.001), postoperative renal dysfunction that required temporary hemodialysis (OR 6.60 95% CI: 1.97-22.11, P=0.002), and re-exploration to stop bleeding (OR 2.65, 95% CI: 1.00-6.99, P=0.050).
Preoperative cardiac tamponade, central arterial cannulation for CPB, postoperative stroke, postoperative renal dysfunction that required temporary hemodialysis, and re-exploration to stop bleeding are perioperative risk factors for delayed extubation. Identification of the potential risk factors for delayed extubation may help optimize the perioperative management and improve postoperative outcomes of patients undergoing ATAAD surgery.
心脏手术后延迟拔管与高发病率和死亡率、重症监护病房住院时间延长以及医疗费用增加相关。急性A型主动脉夹层(ATAAD)由于手术管理的复杂性和一些术后并发症,通常导致机械通气时间延长。本研究旨在阐明ATAAD手术患者延迟拔管的围手术期危险因素。
进行一项回顾性队列研究,纳入2004年10月至2018年1月期间诊断为ATAAD并接受急诊手术的239例患者。收集延迟拔管的潜在围手术期危险因素。本研究将延迟拔管定义为开始拔管时间大于48小时。对临床数据进行单因素和多因素分析,以确定ATAAD手术后延迟拔管的危险因素。
延迟拔管的发生率为48.5%(n = 116)。多因素logistic回归分析显示,延迟拔管的围手术期危险因素包括术前心脏压塞[比值比(OR)3.94,95%置信区间(CI)1.39 - 11.17,P = 0.010]、体外循环(CPB)时中心动脉插管(升主动脉和主动脉弓近端)(OR 4.04,95% CI:1.03 - 15.91,P = 0.046)、术后卒中(OR 10.58,95% CI:2.65 - 42.25,P = 0.001)、术后需要临时血液透析的肾功能不全(OR 6.60,95% CI:1.97 - 22.11,P = 0.002)以及再次手术止血(OR 2.65,95% CI:1.00 - 6.99,P = 0.050)。
术前心脏压塞、CPB时中心动脉插管、术后卒中、术后需要临时血液透析的肾功能不全以及再次手术止血是延迟拔管的围手术期危险因素。识别延迟拔管的潜在危险因素可能有助于优化围手术期管理并改善ATAAD手术患者的术后结局。