Chapman Kenneth B, Van Roosendaal Bert-Kristian W, Van Helmond Noud, Yousef Tariq A
Pain Management, Hofstra Medical School/Northwell Health Systems, New York, USA.
Anesthesiology/Pain Management, New York University Langone Medical Center, New York, USA.
Cureus. 2020 Sep 30;12(9):e10735. doi: 10.7759/cureus.10735.
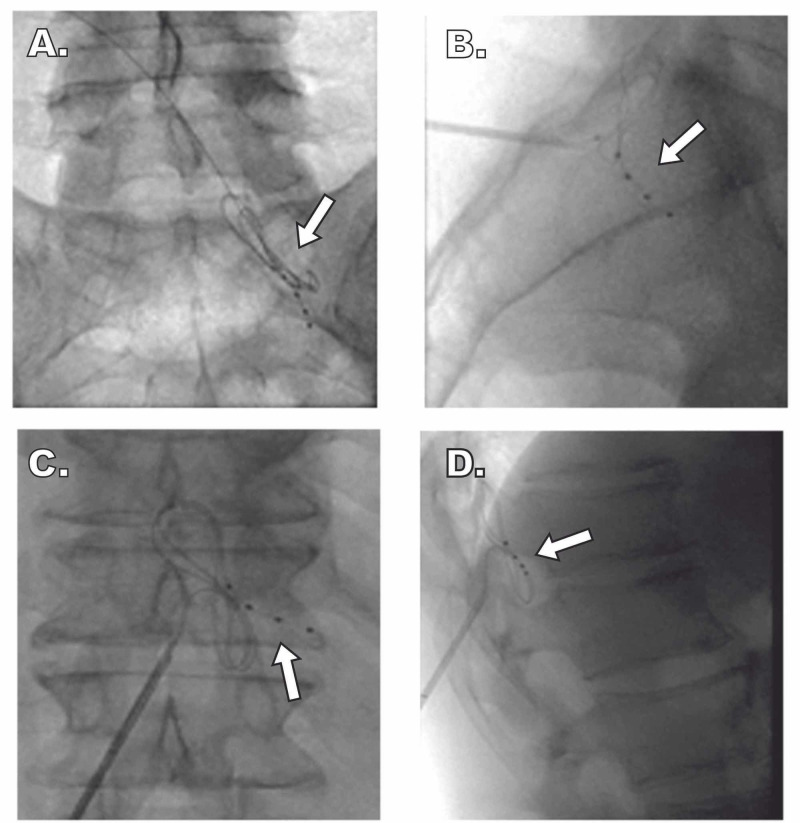
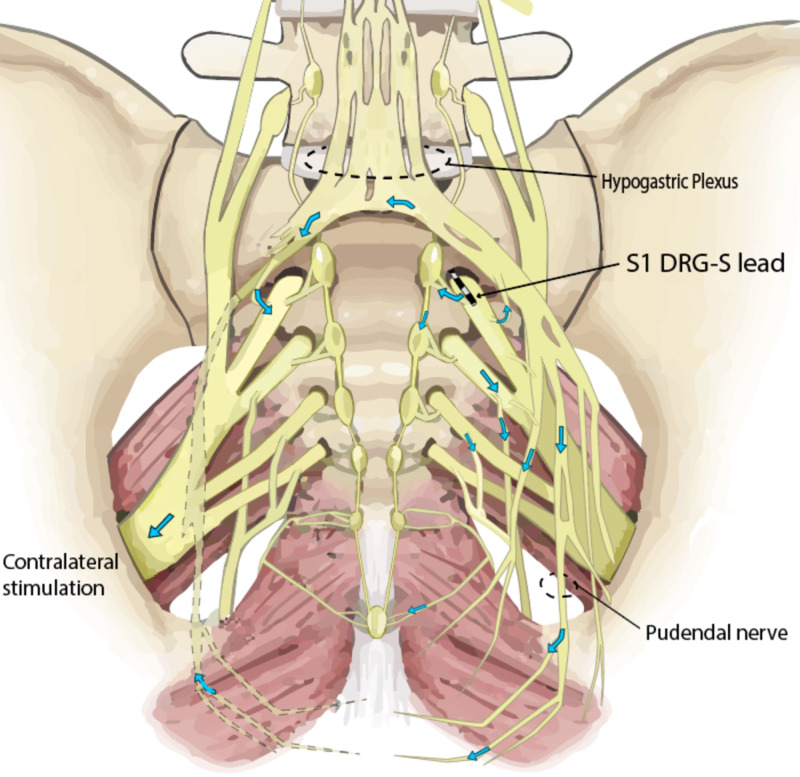
Dorsal root ganglion stimulation (DRG-S) is a form of neuromodulation that can target specific dermatomes to obtain better coverage of the distal extremity. Previously proposed mechanisms of action for DRG-S focused on the dorsal root ganglion (DRG) itself, without consideration of orthodromic effects in the dorsal horn and antidromic effects on the nerve root and sympathetic chain. Diabetic peripheral neuropathy (DPN) is an axonal neuropathy that affects around half of all patients with diabetes mellitus, causing severe pain and sensory impairment in the distal extremities. We present a case of a patient with DPN in both feet, in addition to low back pain, who underwent a DRG-S trial with right T12 and S1 leads. The trial was performed unilaterally for seven days, allowing the patient to compare the treated versus the untreated (left) side. Pain, disability, general health status, and quality of life measures improved significantly. In addition to the significant pain relief in the low back and feet, the patient had near resolution of other DPN-related symptoms, including numbness, bluish discoloration, and allodynia of both feet. He also demonstrated functional and psychological benefits with only a single-sided lead. Overall, the placement of unilateral T12 and S1 DRG-S leads resulted in symmetric improvement of DPN symptoms. A possible mechanism of action is antidromic propagation of action potential signaling into the sympathetic chain to a central ganglion and then to the contralateral sympathetic chain. Given the DRG's ability to directly affect afferent sympathetic fibers with low-frequency stimulation, DRG-S may be an effective neuromodulatory treatment for DPN.
背根神经节刺激(DRG - S)是一种神经调节形式,可靶向特定皮节以更好地覆盖远端肢体。先前提出的DRG - S作用机制主要集中在背根神经节(DRG)本身,而未考虑背角的顺行效应以及对神经根和交感神经链的逆行效应。糖尿病周围神经病变(DPN)是一种轴索性神经病变,影响约一半的糖尿病患者,导致远端肢体严重疼痛和感觉障碍。我们报告一例双足患有DPN且伴有腰痛的患者,该患者接受了右侧T12和S1导联的DRG - S试验。该试验单侧进行了七天,让患者比较治疗侧与未治疗侧(左侧)。疼痛、残疾、总体健康状况和生活质量指标均有显著改善。除了腰背部和足部疼痛明显缓解外,患者其他与DPN相关的症状几乎消失,包括双脚麻木、皮肤发蓝和感觉异常。仅通过单侧导联,他还展现出功能和心理方面的益处。总体而言,单侧T12和S1 DRG - S导联的植入导致DPN症状对称改善。一种可能的作用机制是动作电位信号逆行传播至交感神经链,再到中枢神经节,然后传至对侧交感神经链。鉴于DRG能够通过低频刺激直接影响传入交感神经纤维,DRG - S可能是治疗DPN的一种有效神经调节疗法。