Vickers Donald M, Reddy Arundathi, Akmyradov Chary, Brown Kesley M, Boyanton Bobby L, Wright Heather D, Taylor Jay A, Childress Sherry H, Hartzell Larry D, Johnson Adam B, Key James M, Nolder Abby R, Richter Gresham T, Wineland Andre' M, Strub Graham M
Otolaryngology-Head and Neck Surgery, College of Medicine, University of Arkansas for Medical Sciences, Little Rock, Arkansas, U.S.A.
Pediatric Otolaryngology, Anesthesiology, Pathology and Laboratory Medicine, Arkansas Children's Hospital, Little Rock, Arkansas, U.S.A.
Laryngoscope. 2021 Jun;131(6):E2074-E2079. doi: 10.1002/lary.29236. Epub 2020 Nov 5.
OBJECTIVES/HYPOTHESIS: To determine whether the presence of detectable upper respiratory infections (URIs) at the time of adenoidectomy/adenotonsillectomy is associated with increased morbidity, complications, and unexpected admissions.
Prospective double-blinded cohort.
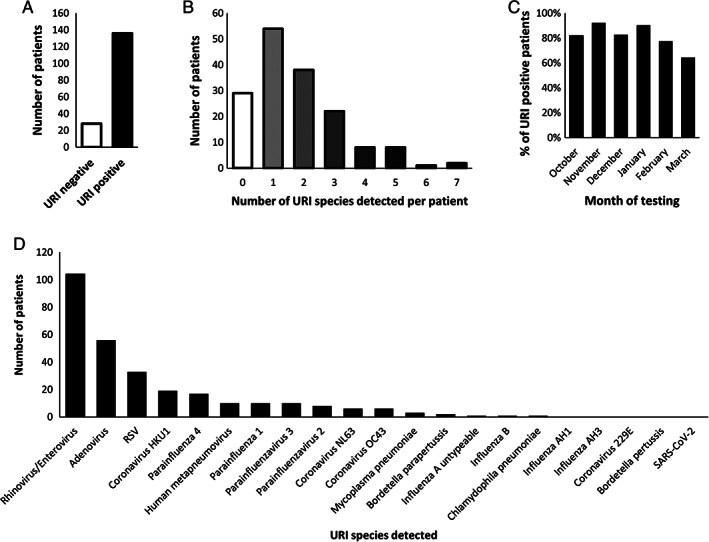
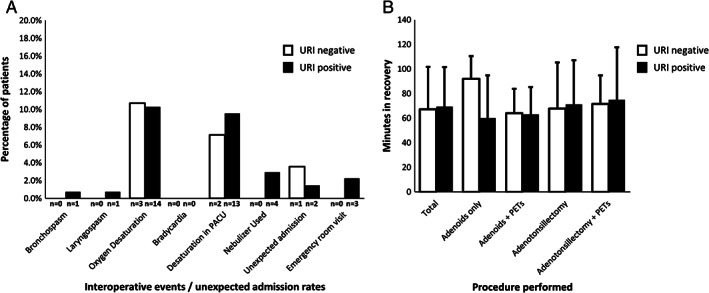
In this prospective cohort study, nasopharyngeal swabs were obtained intraoperatively from 164 pediatric patients undergoing outpatient adenoidectomy/tonsillectomy with or without pressure equalization tubes (PETs) and were analyzed with PCR for the presence of 22 known URIs, including SARS-CoV-2. Surgeons and families were blinded to the results. At the conclusion of the study, rates of detectable infection were determined and intraoperative and postoperative events (unexpected admissions, length of PACU stay, rates of laryngospasm/bronchospasm, oxygen desaturation, bradycardia, and postoperative presentation to an emergency department) were compared between infected and uninfected patients.
Of the 164 patients (50% male, 50% female, ages 8 mo-18 y), 136 patients (82.9%) tested positive for one or more URI at the time of surgery. Forty one patients (25.0%) tested positive for three or more URIs concurrently, and 11 (6.7%) tested positive for five or more URIs concurrently. There were no significant differences in admission rates, length of PACU stay, rates of laryngospasm/bronchospasm, oxygen desaturation, bradycardia, or postoperative presentation to an emergency department between positive and negative patients. No patients tested positive for SARS-CoV-2.
A recent positive URI test does not confer any additional intraoperative or postoperative risk in the setting of outpatient adenoidectomy/tonsillectomy in healthy patients. There is no utility in preoperative URI testing, and delaying surgery due to a recent positive URI test is not warranted in this population.
3 Laryngoscope, 131:E2074-E2079, 2021.
目的/假设:确定腺样体切除术/腺样体扁桃体切除术时可检测到的上呼吸道感染(URI)是否与发病率增加、并发症及意外入院有关。
前瞻性双盲队列研究。
在这项前瞻性队列研究中,术中从164例接受门诊腺样体切除术/扁桃体切除术(伴或不伴鼓膜通气管[PET])的儿科患者中获取鼻咽拭子,并用聚合酶链反应(PCR)分析22种已知URI的存在情况,包括严重急性呼吸综合征冠状病毒2(SARS-CoV-2)。外科医生和家属对结果不知情。在研究结束时,确定可检测到的感染率,并比较感染患者和未感染患者的术中及术后事件(意外入院、麻醉后监护病房[PACU]停留时间、喉痉挛/支气管痉挛发生率、氧饱和度下降、心动过缓以及术后到急诊科就诊情况)。
164例患者(50%为男性,50%为女性,年龄8个月至18岁)中,136例患者(82.9%)在手术时一种或多种URI检测呈阳性。41例患者(25.0%)同时三种或更多种URI检测呈阳性,11例患者(6.7%)同时五种或更多种URI检测呈阳性。阳性患者和阴性患者在入院率、PACU停留时间、喉痉挛/支气管痉挛发生率、氧饱和度下降、心动过缓或术后到急诊科就诊方面无显著差异。无患者SARS-CoV-2检测呈阳性。
近期URI检测呈阳性在健康患者门诊腺样体切除术/扁桃体切除术中不会带来额外的术中或术后风险。术前进行URI检测没有用处,且该人群中因近期URI检测呈阳性而推迟手术没有必要。
3《喉镜》,131:E2074 - E2079,2021年。