Amarenco Pierre, Denison Hans, Evans Scott R, Himmelmann Anders, James Stefan, Knutsson Mikael, Ladenvall Per, Molina Carlos A, Wang Yongjun, Johnston S Claiborne
Department of Neurology and Stroke Center, Bichat University Hospital, University of Paris, Paris, France.
AstraZeneca, Biopharmaceuticals R&D, Gothenburg, Sweden.
JAMA Neurol. 2020 Nov 7;78(2):1-9. doi: 10.1001/jamaneurol.2020.4396.
Reduction of subsequent disabling stroke is the main goal of preventive treatment in the acute setting after transient ischemic attack (TIA) or minor ischemic stroke.
To evaluate the superiority of ticagrelor added to aspirin in preventing disabling stroke and to understand the factors associated with recurrent disabling stroke.
DESIGN, SETTING, AND PARTICIPANTS: The Acute Stroke or Transient Ischemic Attack Treated With Ticagrelor and Aspirin for Prevention of Stroke and Death (THALES) was a randomized clinical trial conducted between January 22, 2018, and December 13, 2019, with a 30-day follow-up, at 414 hospitals in 28 countries. The trial included 11 016 patients with a noncardioembolic, nonsevere ischemic stroke or high-risk TIA, including 10 803 with modified Rankin Scale score (mRS) recorded at 30 days.
Ticagrelor (180-mg loading dose on day 1 followed by 90 mg twice daily for days 2-30) or placebo within 24 hours of symptom onset. All patients received aspirin, 300 to 325 mg on day 1 followed by 75 to 100 mg daily for days 2 to 30.
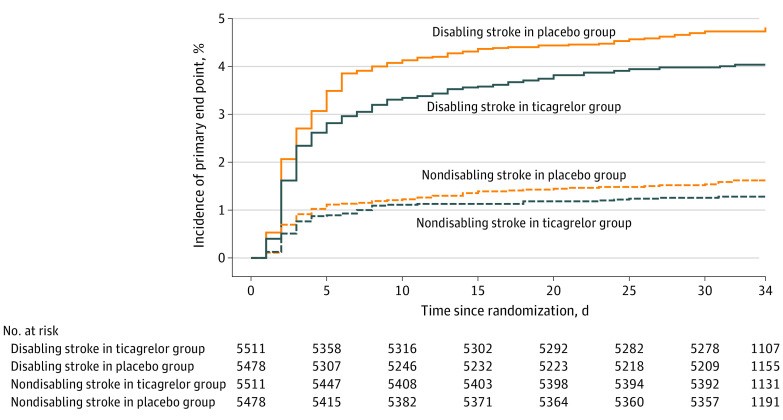
Time to the occurrence of disabling stroke (progression of index event or new stroke) or death within 30 days, as measured by mRS at day 30. Disabling stroke was defined by mRS greater than 1.
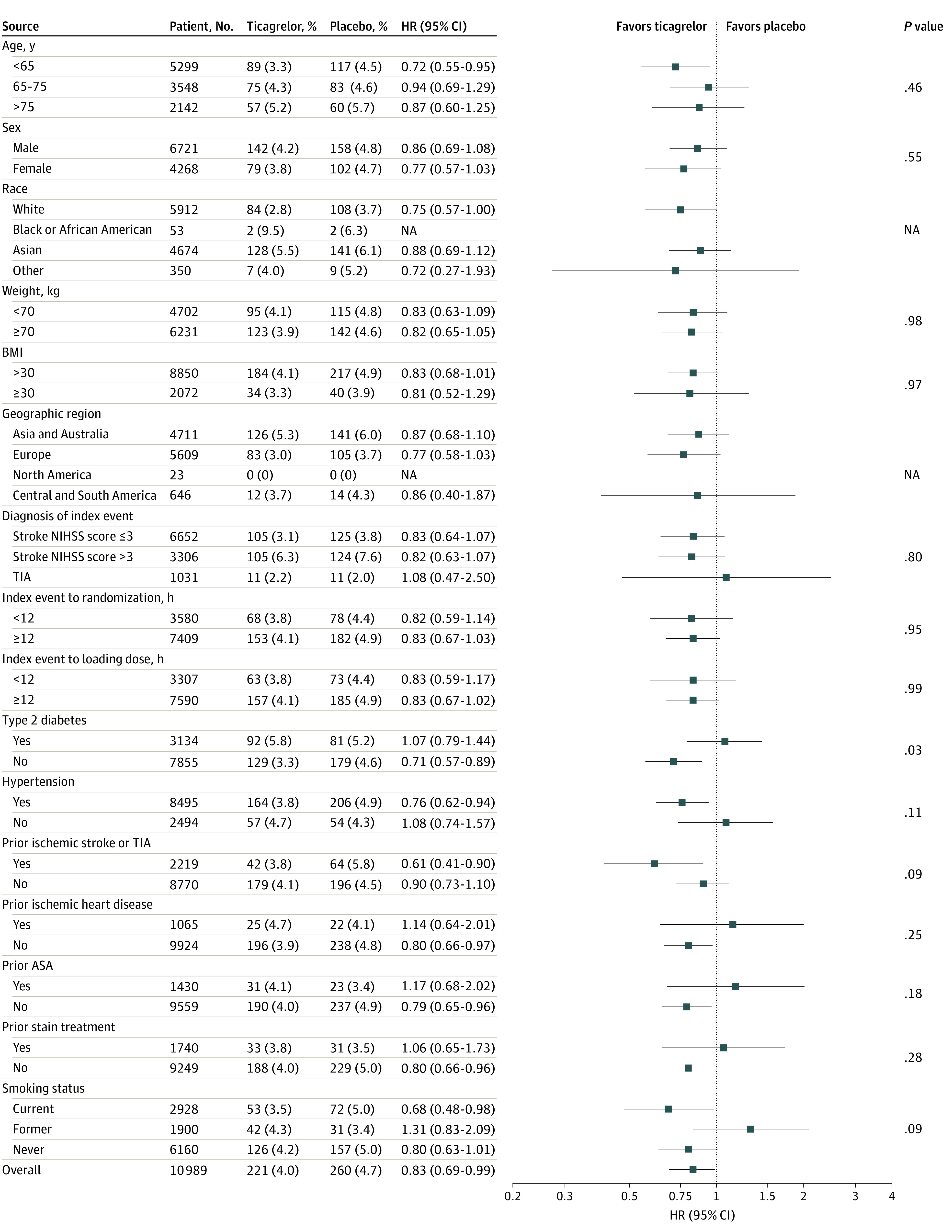
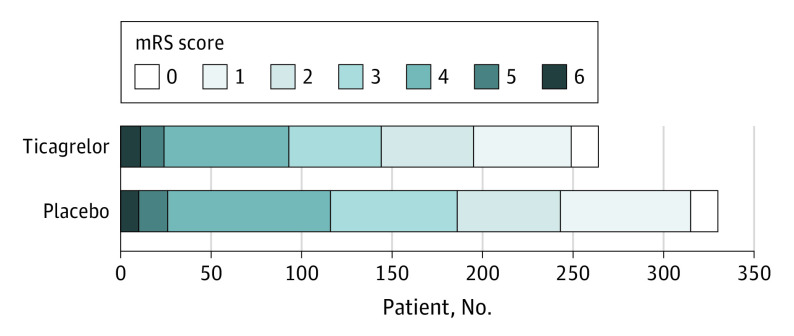
Among participants with 30-day mRS greater than 1, mean age was 68.1 years, 1098 were female (42.6%), and 2670 had an ischemic stroke (95.8%) as a qualifying event. Among 11 016 patients, a primary end point with mRS greater than 1 at 30 days occurred in 221 of 5511 patients (4.0%) randomized to ticagrelor and in 260 of 5478 patients (4.7%) randomized to placebo (hazard ratio [HR], 0.83; 95% CI, 0.69-0.99, P = .04). A primary end point with mRS 0 or 1 at 30 days occurred in 70 of 5511 patients (1.3%) and 87 of 5478 patients (1.6%) (HR, 0.79; 95% CI, 0.57-1.08; P = .14). The ordinal analysis of mRS in patients with recurrent stroke showed a shift of the disability burden following a recurrent ischemic stroke in favor of ticagrelor (odds ratio, 0.77; 95% CI, 0.65-0.91; P = .002). Factors associated with disability were baseline National Institutes of Health Stroke Scale score 4 to 5, ipsilateral stenosis of at least 30%, Asian race/ethnicity, older age, and higher systolic blood pressure, while treatment with ticagrelor was associated with less disability.
In patients with TIA and minor ischemic stroke, ticagrelor added to aspirin was superior to aspirin alone in preventing disabling stroke or death at 30 days and reduced the total burden of disability owing to ischemic stroke recurrence.
ClinicalTrials.gov Identifier: NCT03354429.
减少随后发生的致残性中风是短暂性脑缺血发作(TIA)或轻度缺血性中风后急性治疗中的主要预防目标。
评估替格瑞洛联合阿司匹林在预防致残性中风方面的优越性,并了解与复发性致残性中风相关的因素。
设计、设置和参与者:替格瑞洛和阿司匹林治疗预防中风和死亡的急性中风或短暂性脑缺血发作(THALES)是一项随机临床试验,于2018年1月22日至2019年12月13日进行,为期30天随访,在28个国家的414家医院开展。该试验纳入了11016例非心源性、非严重缺血性中风或高危TIA患者,其中10803例在30天时记录了改良Rankin量表评分(mRS)。
症状发作后24小时内给予替格瑞洛(第1天负荷剂量180mg,随后第2 - 30天每日两次,每次90mg)或安慰剂。所有患者均接受阿司匹林治疗,第1天300 - 325mg,随后第2 - 30天每日75 - 100mg。
30天内发生致残性中风(索引事件进展或新发中风)或死亡的时间,通过第30天的mRS进行测量。致残性中风定义为mRS大于1。
在30天mRS大于1的参与者中,平均年龄为68.1岁,1098例为女性(42.6%),2670例以缺血性中风(95.8%)作为符合条件的事件。在11016例患者中,随机接受替格瑞洛治疗的5511例患者中有221例(4.0%)在30天时出现mRS大于1的主要终点,随机接受安慰剂治疗的5478例患者中有260例(4.7%)出现该终点(风险比[HR],0.83;95%置信区间[CI],0.69 - 0.99,P = 0.04)。在30天时mRS为0或1的主要终点在5511例患者中有70例(1.3%),在5478例患者中有87例(1.6%)(HR,0.79;95%CI,0.57 - 1.08;P = 0.14)。复发性中风患者mRS的序贯分析显示,复发性缺血性中风后残疾负担的变化有利于替格瑞洛(优势比,0.77;95%CI,0.65 - 0.91;P = 0.002)。与残疾相关的因素包括基线美国国立卫生研究院卒中量表评分为4至5分、同侧狭窄至少30%、亚洲种族/族裔、年龄较大以及收缩压较高,而替格瑞洛治疗与较少的残疾相关。
在TIA和轻度缺血性中风患者中,替格瑞洛联合阿司匹林在预防30天内致残性中风或死亡方面优于单用阿司匹林,并降低了缺血性中风复发导致的总残疾负担。
ClinicalTrials.gov标识符:NCT03354429。