Assistance Publique - Hôpitaux de Marseille, Hôpital Nord, Médecine Intensive Réanimation, 13015, Marseille, France.
Faculté de médecine, Groupe de recherche en Réanimation et Anesthésie de Marseille pluridisciplinaire (GRAM +), Centre d'Etudes et de Recherches sur les Services de Santé et qualité de vie EA 3279, Aix-Marseille Université, 13005, Marseille, France.
Intensive Care Med. 2020 Dec;46(12):2357-2372. doi: 10.1007/s00134-020-06297-8. Epub 2020 Nov 7.
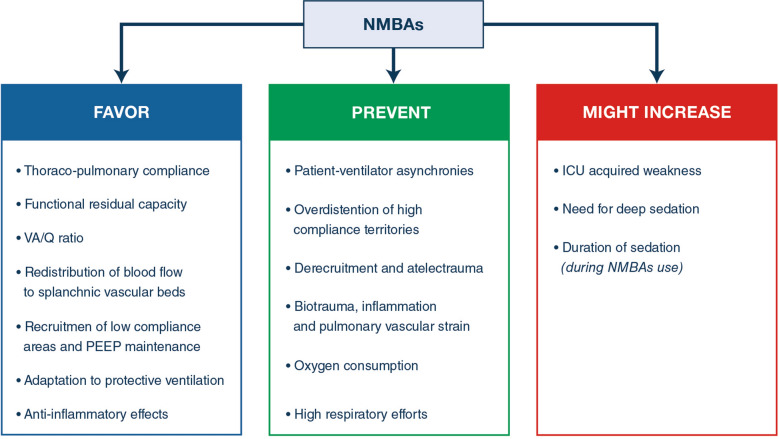
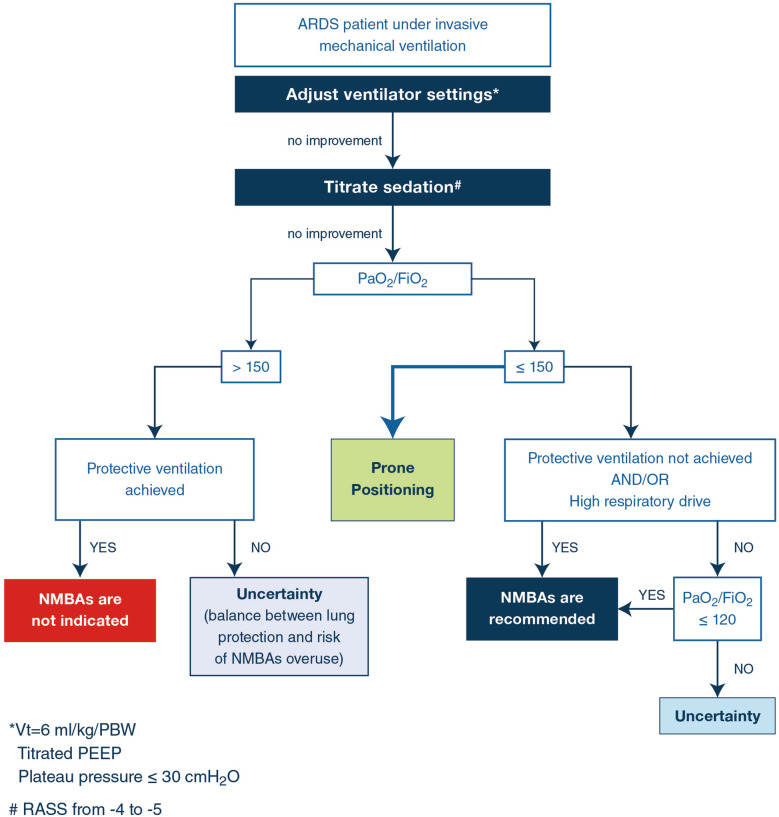
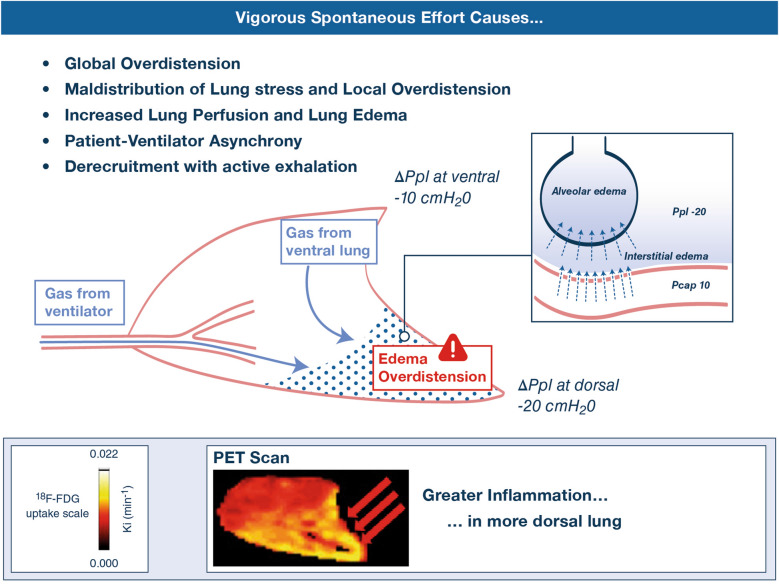
Neuromuscular blocking agents (NMBAs) inhibit patient-initiated active breath and the risk of high tidal volumes and consequent high transpulmonary pressure swings, and minimize patient/ ventilator asynchrony in acute respiratory distress syndrome (ARDS). Minimization of volutrauma and ventilator-induced lung injury (VILI) results in a lower incidence of barotrauma, improved oxygenation and a decrease in circulating proinflammatory markers. Recent randomized clinical trials did not reveal harmful muscular effects during a short course of NMBAs. The use of NMBAs should be considered during the early phase of severe ARDS for patients to facilitate lung protective ventilation or prone positioning only after optimising mechanical ventilation and sedation. The use of NMBAs should be integrated in a global strategy including the reduction of tidal volume, the rational use of PEEP, prone positioning and the use of a ventilatory mode allowing spontaneous ventilation as soon as possible. Partial neuromuscular blockade should be evaluated in future trials.
神经肌肉阻滞剂(NMBAs)抑制患者主动呼吸,并降低潮气量和跨肺压波动的风险,最小化急性呼吸窘迫综合征(ARDS)患者与呼吸机的不同步。减少肺容积伤和呼吸机相关性肺损伤(VILI)可降低气压伤的发生率,改善氧合,并降低循环促炎标志物的水平。最近的随机临床试验并未显示在使用 NMBA 的短期疗程中有有害的肌肉效应。对于严重 ARDS 患者,只有在优化机械通气和镇静后,才应考虑在早期使用 NMBA 来辅助肺保护性通气或俯卧位通气。NMBA 的使用应整合在一个整体策略中,包括降低潮气量、合理使用 PEEP、俯卧位和使用允许尽快自主通气的通气模式。未来的试验应评估部分神经肌肉阻滞。