Division of Infectious Diseases, Department of Medicine, Duke University Medical Center, Durham, North Carolina, United States of America.
PLoS One. 2020 Nov 9;15(11):e0242055. doi: 10.1371/journal.pone.0242055. eCollection 2020.
Novel approaches are required to better focus latent tuberculosis infection (LTBI) efforts in low-prevalence regions. Geographic information systems, used within large health systems, may provide one such approach.
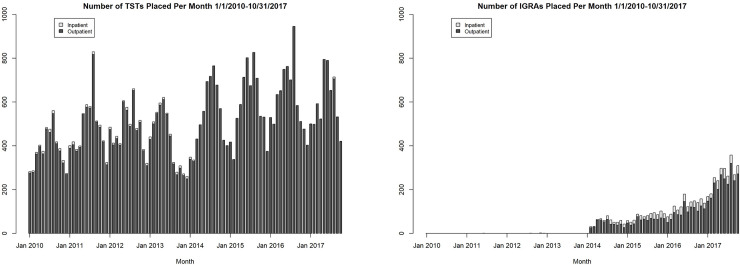
A retrospective, cross-sectional design was used to integrate US Census and Duke Health System data between January 1, 2010 and October 31, 2017 and examine the relationships between LTBI screening and population tuberculosis risk (assessed using the surrogate measure of proportion of persons born in tuberculosis-endemic regions) by census tract.
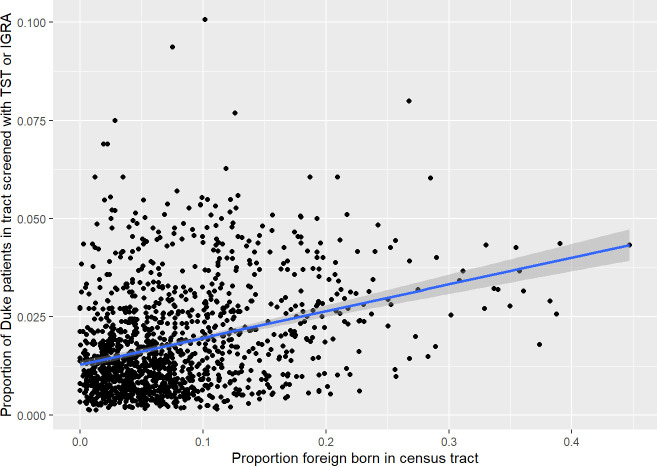
The median proportion of Duke patients screened per census tract was 0.01 (range 0-0.1, interquartile range 0.01-0.03). The proportion of Duke patients screened within a census tract significantly but weakly correlated with the population risk. Furthermore, patients residing in census tracts with higher population tuberculosis risk were more likely to be screened with TST than with an IGRA (p<0.001).
The weak correlation between patient proportion screened for LTBI and our surrogate marker of population tuberculosis risk suggests that LTBI screening efforts should be better targeted. This type of geography-based analysis may serve as an easily obtainable benchmark for LTBI screening in health systems with low tuberculosis prevalence.
需要新的方法来更好地集中在低患病率地区的潜伏性结核病感染(LTBI)工作。地理信息系统,在大型卫生系统中使用,可能提供这样的一种方法。
采用回顾性、横断面设计,整合了 2010 年 1 月 1 日至 2017 年 10 月 31 日期间的美国人口普查和杜克健康系统数据,并通过普查区检查 LTBI 筛查与人群结核病风险(使用出生于结核病流行地区的比例的替代指标评估)之间的关系。
每个普查区筛查的杜克患者中位数比例为 0.01(范围 0-0.1,四分位距 0.01-0.03)。普查区内筛查的杜克患者比例与人群风险显著但弱相关。此外,居住在人群结核病风险较高的普查区的患者更有可能接受 TST 筛查而不是 IGRA(p<0.001)。
LTBI 筛查患者比例与我们的人群结核病风险替代标志物之间的弱相关性表明,LTBI 筛查工作应更好地针对目标人群。这种基于地理的分析类型可以作为低结核病患病率卫生系统中 LTBI 筛查的一个易于获得的基准。