Division of Infectious Diseases, Department of Internal Medicine Santa Casa de São Paulo School of Medical Sciences, Hospital da Irmandade da Santa Casa de Misericórdia de São Paulo, Rua Dr Cesáreo Mota Jr 112,, São Paulo, SP, CEP: 01303-060, Brazil.
Emílio Ribas Institute of Infectious Diseases, Av Dr Arnaldo 165, São Paulo, SP, CEP: 01246-900, Brazil.
BMC Infect Dis. 2018 Nov 19;18(1):585. doi: 10.1186/s12879-018-3508-8.
In developing countries, tuberculosis (TB) is a major public health problem and the leading cause of death among patients with HIV (Human Immunodeficiency Virus). Until 2001, the tuberculin skin test (TST) was the only available tool for the diagnosis of latent tuberculosis infection (LTBI), but false-negative TST results are frequently reported. Recently, the interferon-γ (IFN-γ) release assay (IGRA) has gained ground because it can detect the IFN-γ secreted by circulating lymphocytes T cells when stimulated by specific TB antigens. However, the role of IGRA in the diagnosis of LTBI in HIV-infected patients has not been well established.
This cross-sectional study compared the accuracy of TST (performed by the Mantoux method) and IGRA (QuantiFERON-TB Gold In-Tube, Cellestis, Carnegie, Australia) on the diagnosis of LTBI among patients with HIV. LTBI is defined by LTBI risk and at least one positive test (TST or IGRA), without clinical evidence of active TB. We also assessed the accuracy of TST and IGRA among HIV patients with high and low risk for LTBI.
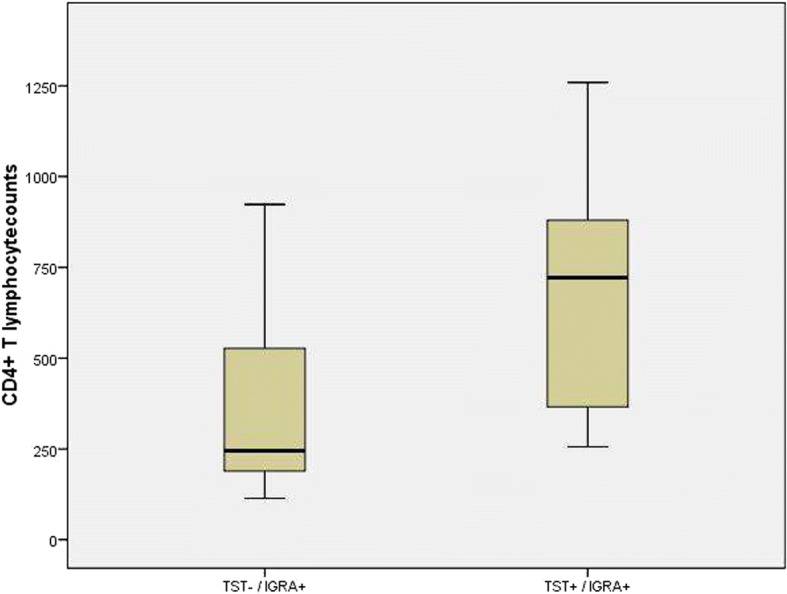
Among 90 HIV patients, 80 met the study criteria for LTBI, fifty-nine (73.7%) patients were TST positive, 21 (26.2%) were negative, whereas 75 patients (93.7%) were IGRA positive, and five (6.2%) were negative. TST showed poor agreement with the diagnosis of LTBI (Kappa: 0.384), while IGRA demonstrated good agreement (Kappa: 0.769). Among 69 patients with high risk and 21 with low risk for LTBI, TST was positive in 48 (69.5%) and 11 (52.4%), while IGRA was positive in 68 (98.5%) and 7 (33.3%) patients, respectively. There were no association between TST and the level of risk (P = 0,191). Conversely, we observed a strong association between the IGRA and risk for LTBI (p < 0.001).
Compared to TST, IGRA positivity is consistent with the risk of TB infection and seems to be a better diagnostic tool for LTBI in HIV-infected patients.
在发展中国家,结核病(TB)是一个主要的公共卫生问题,也是 HIV(人类免疫缺陷病毒)感染者的主要死亡原因。直到 2001 年,结核菌素皮肤试验(TST)是诊断潜伏性结核感染(LTBI)的唯一可用工具,但经常有假阴性 TST 结果的报道。最近,γ-干扰素(IFN-γ)释放检测(IGRA)得到了广泛应用,因为它可以检测到当循环淋巴细胞 T 细胞受到特定的 TB 抗原刺激时分泌的 IFN-γ。然而,IGRA 在诊断 HIV 感染者中的 LTBI 中的作用尚未得到很好的确定。
这项横断面研究比较了 TST(采用曼托氏法)和 IGRA(QuantiFERON-TB Gold In-Tube,Cellestis,Carnegie,Australia)在诊断 HIV 感染者中的 LTBI 的准确性。LTBI 是指通过 LTBI 风险和至少一项阳性检测(TST 或 IGRA)定义的,没有活动性 TB 的临床证据。我们还评估了 TST 和 IGRA 在 LTBI 高危和低危的 HIV 患者中的准确性。
在 90 名 HIV 患者中,有 80 名符合 LTBI 的研究标准,59 名(73.7%)患者 TST 阳性,21 名(26.2%)阴性,而 75 名(93.7%)患者 IGRA 阳性,5 名(6.2%)阴性。TST 与 LTBI 的诊断一致性较差(Kappa:0.384),而 IGRA 则具有较好的一致性(Kappa:0.769)。在 69 名高危和 21 名低危 LTBI 患者中,TST 阳性分别为 48 名(69.5%)和 11 名(52.4%),而 IGRA 阳性分别为 68 名(98.5%)和 7 名(33.3%)。TST 与风险水平之间没有相关性(P=0.191)。相反,我们观察到 IGRA 与 LTBI 风险之间存在很强的相关性(p<0.001)。
与 TST 相比,IGRA 阳性与 TB 感染的风险一致,似乎是 HIV 感染者 LTBI 的更好的诊断工具。