Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, South Korea.
Department of Internal Medicine, Seoul National University College of Medicine, Seoul, South Korea.
J Am Soc Nephrol. 2021 Jan;32(1):199-210. doi: 10.1681/ASN.2019050546. Epub 2020 Nov 9.
Tacrolimus is used as a steroid-sparing immunosuppressant in adults with minimal change nephrotic syndrome. However, combined treatment with tacrolimus and low-dose steroid has not been compared with high-dose steroid for induction of clinical remission in a large-scale randomized study.
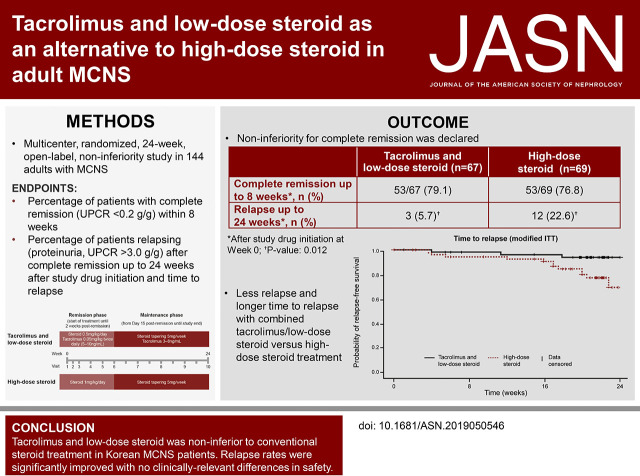
In this 24-week open-label noninferiority study, we randomized 144 adults with minimal change nephrotic syndrome to receive 0.05 mg/kg twice-daily tacrolimus plus once-daily 0.5 mg/kg prednisolone, or once-daily 1 mg/kg prednisolone alone, for up to 8 weeks or until achieving complete remission. Two weeks after complete remission, we tapered the steroid to a maintenance dose of 5-7.5 mg/d in both groups until 24 weeks after study drug initiation. The primary end point was complete remission within 8 weeks (urine protein: creatinine ratio <0.2 g/g). Secondary end points included time until remission and relapse rates (proteinuria and urine protein: creatinine ratio >3.0 g/g) after complete remission to within 24 weeks of study drug initiation.
Complete remission within 8 weeks occurred in 53 of 67 patients (79.1%) receiving tacrolimus and low-dose steroid and 53 of 69 patients (76.8%) receiving high-dose steroid; this difference demonstrated noninferiority, with an upper confidence limit below the predefined threshold (20%) in both intent-to-treat (11.6%) and per-protocol (17.0%) analyses. Groups did not significantly differ in time until remission. Significantly fewer patients relapsed on maintenance tacrolimus (3-8 ng/ml) plus tapered steroid versus tapered steroid alone (5.7% versus 22.6%, respectively; =0.01). There were no clinically relevant safety differences.
Combined tacrolimus and low-dose steroid was noninferior to high-dose steroid for complete remission induction in adults with minimal change nephrotic syndrome. Relapse rates were significantly lower with maintenance tacrolimus and steroid compared with steroid alone. No clinically-relevant differences in safety findings were observed.
他克莫司被用作成人微小病变肾病综合征的类固醇免疫抑制剂。然而,在大规模随机研究中,他克莫司与低剂量类固醇联合治疗与高剂量类固醇诱导临床缓解的效果尚未进行比较。
在这项为期 24 周的开放性非劣效性研究中,我们将 144 名微小病变肾病综合征的成年人随机分为两组,分别接受每日两次 0.05mg/kg 的他克莫司联合每日一次 0.5mg/kg 的泼尼松龙,或单独每日一次 1mg/kg 的泼尼松龙治疗,持续 8 周或直至完全缓解。完全缓解后 2 周,两组患者均将类固醇逐渐减至维持剂量 5-7.5mg/d,直至研究药物起始后 24 周。主要终点为 8 周内完全缓解(尿蛋白与肌酐比值<0.2g/g)。次要终点包括完全缓解后至研究药物起始后 24 周内的缓解时间和复发率(蛋白尿和尿蛋白与肌酐比值>3.0g/g)。
接受他克莫司和低剂量类固醇治疗的 67 名患者中有 53 名(79.1%)和接受高剂量类固醇治疗的 69 名患者中有 53 名(76.8%)在 8 周内完全缓解;意向治疗(11.6%)和方案治疗(17.0%)分析的上限置信区间均低于预设阈值(20%),表明这两种治疗方案无差异。两组患者的缓解时间无显著差异。维持治疗(3-8ng/ml)时联合使用他克莫司和逐渐减少的类固醇治疗的患者复发率显著低于单独使用类固醇的患者(分别为 5.7%和 22.6%,P=0.01)。两种治疗方案的安全性差异无临床意义。
在成人微小病变肾病综合征患者中,他克莫司联合低剂量类固醇与高剂量类固醇诱导完全缓解的效果无差异。与单独使用类固醇相比,使用维持治疗(3-8ng/ml)的他克莫司和逐渐减少的类固醇治疗的患者复发率显著降低。在安全性方面,未观察到具有临床意义的差异。